Anda mungkin juga menyukai
- 2009 Esc GuidelinesperioperativecardiaccareDokumen44 halaman2009 Esc GuidelinesperioperativecardiaccareAgnese ValentiniBelum ada peringkat
- ESPEN GuidelineDokumen37 halamanESPEN GuidelineAuliangi TamayoBelum ada peringkat
- 100 BLWrecipesDokumen52 halaman100 BLWrecipeslona2010100% (1)
- Managing Coagulopathy ICUDokumen38 halamanManaging Coagulopathy ICUMirabela Colac100% (1)
- 00.QUICK GUIDE TO Cardiopulmonary Care 3rd PDFDokumen246 halaman00.QUICK GUIDE TO Cardiopulmonary Care 3rd PDFMirabela ColacBelum ada peringkat
- Ventilator Final Version 180215Dokumen64 halamanVentilator Final Version 180215Mirabela ColacBelum ada peringkat
- Ultrasound Guidance - PollardDokumen72 halamanUltrasound Guidance - Pollardmasquebolso100% (3)
- HSRP 04 153Dokumen15 halamanHSRP 04 153Mirabela ColacBelum ada peringkat
- ARDSnet Ventilation Protocol SummaryDokumen2 halamanARDSnet Ventilation Protocol SummaryvbfisioBelum ada peringkat
- Anesthesia GuideDokumen84 halamanAnesthesia GuideRaisa Paz RamosBelum ada peringkat
- 05 OA - 033-0911 - Koh Liang Khai DarrenDokumen7 halaman05 OA - 033-0911 - Koh Liang Khai DarrenMirabela ColacBelum ada peringkat
- Ten Things To Know - Stroke Guidelinesv1Dokumen1 halamanTen Things To Know - Stroke Guidelinesv1Mirabela ColacBelum ada peringkat
- 168 Antibiotics in Critical Care - An IntroductionDokumen6 halaman168 Antibiotics in Critical Care - An IntroductionMirabela ColacBelum ada peringkat
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- MS Case PresDokumen33 halamanMS Case PresShaine_Thompso_6877Belum ada peringkat
- Jcpe 12206 PDFDokumen17 halamanJcpe 12206 PDFrozh rasulBelum ada peringkat
- How To Whistle Loud 14 Steps (With Pictures) - WikiHowDokumen4 halamanHow To Whistle Loud 14 Steps (With Pictures) - WikiHowVeselin VasilevBelum ada peringkat
- ENT Radiology ADokumen64 halamanENT Radiology AMitulsinh M RavaljiBelum ada peringkat
- Free Printable at Home Brain Breaks and Active CalmingDokumen12 halamanFree Printable at Home Brain Breaks and Active Calmingapi-505036826Belum ada peringkat
- Passive to Active Voice ConversionDokumen3 halamanPassive to Active Voice ConversionQhaisya Binasanjaya67% (3)
- Location and External Anatomy of The KidneysDokumen15 halamanLocation and External Anatomy of The KidneysKyla Malapit GarvidaBelum ada peringkat
- Lecture 3 - Monod KineticsDokumen19 halamanLecture 3 - Monod KineticsZeny Naranjo0% (1)
- The Stages of Mitosis and Meiosis Cell DivisionDokumen50 halamanThe Stages of Mitosis and Meiosis Cell DivisionRosana Beatrix GualbertoBelum ada peringkat
- Human Body System WorksheetDokumen2 halamanHuman Body System WorksheetRPh Krishna Chandra JagritBelum ada peringkat
- jm800328v PDFDokumen9 halamanjm800328v PDFVINODBelum ada peringkat
- Full Lab ReportDokumen5 halamanFull Lab ReportchampmorganBelum ada peringkat
- Answer Guide For O Level Biology (5090/3) - Paper 3 Practical Test June 2001Dokumen3 halamanAnswer Guide For O Level Biology (5090/3) - Paper 3 Practical Test June 2001MSHBelum ada peringkat
- Cell Division MCQ Questions & AnswersDokumen17 halamanCell Division MCQ Questions & Answersmurali.prionsgm100% (1)
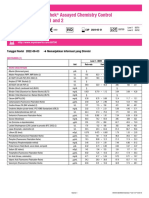
- Lyphochek Assayed Chemistry Control Levels 1 and 2: Tanggal Revisi 2022-06-03 Menunjukkan Informasi Yang DirevisiDokumen2 halamanLyphochek Assayed Chemistry Control Levels 1 and 2: Tanggal Revisi 2022-06-03 Menunjukkan Informasi Yang DirevisiFahmiBelum ada peringkat
- 9700 w01 Ms 2Dokumen4 halaman9700 w01 Ms 2Sathya Seelan0% (1)
- Photosynthesis WorksheetDokumen3 halamanPhotosynthesis WorksheetByambazaya E100% (2)
- Mod 7 PoisoningDokumen12 halamanMod 7 Poisoningrez198767% (3)
- Imaging Modalities For Lung DiseasesDokumen14 halamanImaging Modalities For Lung DiseasesYnaffit Alteza Untal100% (1)
- Pre-Dental Jaw Relationship ReportDokumen10 halamanPre-Dental Jaw Relationship ReportFidz LiankoBelum ada peringkat
- Passion and Deceit Part VI PDFDokumen20 halamanPassion and Deceit Part VI PDFno2meBelum ada peringkat
- Clinic VisitDokumen5 halamanClinic VisitEka YunusBelum ada peringkat
- 15 Healing Miracles EX735 SCENAR Book StoriesDokumen11 halaman15 Healing Miracles EX735 SCENAR Book StoriesBacean Aurel Ioan100% (5)
- Shanks 1996Dokumen5 halamanShanks 1996Sarly FebrianaBelum ada peringkat
- THYMUS PPT Final 7marDokumen15 halamanTHYMUS PPT Final 7marRajesh UgalmugleBelum ada peringkat
- O Treinamento Físico Atenua A Cardiomiopatia Cirrótica (TRADUZIR)Dokumen11 halamanO Treinamento Físico Atenua A Cardiomiopatia Cirrótica (TRADUZIR)Igor Ferrari StreitBelum ada peringkat
- Potato Poisoning: Understanding Solanine ToxicityDokumen13 halamanPotato Poisoning: Understanding Solanine ToxicityDaz Jones100% (2)
- A Simplified Technique For Determining The Occlusal Plane in Full Denture ConstructionDokumen4 halamanA Simplified Technique For Determining The Occlusal Plane in Full Denture ConstructionAlejandro García ArmentaBelum ada peringkat
- Memory SkillsDokumen70 halamanMemory SkillsAsiri Samanatha Elegoda100% (1)
- Cardiology MCQDokumen12 halamanCardiology MCQAhmed MahanaBelum ada peringkat