Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5784)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- B29061KDokumen13 halamanB29061KMeethuanBelum ada peringkat
- Transmission Substation Work Practice Manual 2016-07-22Dokumen499 halamanTransmission Substation Work Practice Manual 2016-07-22Edmund YoongBelum ada peringkat
- BSHF-101 E.MDokumen8 halamanBSHF-101 E.MRajni KumariBelum ada peringkat
- Legalizing abortion in the Philippines for women's health and rightsDokumen2 halamanLegalizing abortion in the Philippines for women's health and rightsRosario Antoniete R. Cabilin100% (1)
- Pregnancy Calendar For DogsDokumen3 halamanPregnancy Calendar For DogsVina Esther FiguraBelum ada peringkat
- Kaplan Grade OverviewDokumen5 halamanKaplan Grade Overviewapi-310875630Belum ada peringkat
- Master Plan for Trivandrum City 2021-2031Dokumen21 halamanMaster Plan for Trivandrum City 2021-2031Adhithy MenonBelum ada peringkat
- A Case of Eclectic Family TherapyDokumen88 halamanA Case of Eclectic Family Therapygun gorBelum ada peringkat
- Report On Legal Medicine PowerpointDokumen31 halamanReport On Legal Medicine PowerpointEdwin VillaBelum ada peringkat
- MMI4804 Quiz 5Dokumen16 halamanMMI4804 Quiz 5Ham Mad0% (1)
- Everything You Need to Know About Prenatal CareDokumen5 halamanEverything You Need to Know About Prenatal Carelaura fernandiaBelum ada peringkat
- Experential and Relationship Oriented Approaches 1Dokumen12 halamanExperential and Relationship Oriented Approaches 1Mary Ann CabalejoBelum ada peringkat
- Ba - Bacterial Identification Lab WorksheetDokumen12 halamanBa - Bacterial Identification Lab WorksheetFay SBelum ada peringkat
- Tailored Health Plans Table of CoverDokumen22 halamanTailored Health Plans Table of CoverAneesh PrabhakaranBelum ada peringkat
- Portal Hypertension Clinical Features and ManagementDokumen29 halamanPortal Hypertension Clinical Features and ManagementPhilip LingBelum ada peringkat
- UK Requirements Checklist and Study MaterialsDokumen2 halamanUK Requirements Checklist and Study MaterialsKrizle AdazaBelum ada peringkat
- WORKPLACE TB POLICYDokumen4 halamanWORKPLACE TB POLICYGigi CabanaBelum ada peringkat
- MudreDokumen10 halamanMudrejezebelvertBelum ada peringkat
- Hypertension Drugs Cheat Sheet: by ViaDokumen3 halamanHypertension Drugs Cheat Sheet: by ViaGulzaib KhokharBelum ada peringkat
- Chirangi vs. StateDokumen3 halamanChirangi vs. StateFaithBelum ada peringkat
- Isolation and Identification of Bacteria ThesisDokumen7 halamanIsolation and Identification of Bacteria Thesisafbtbegxe100% (2)
- Angle Grinder PDFDokumen2 halamanAngle Grinder PDFcityofdarwingisBelum ada peringkat
- College Women's Experiences With Physically Forced, Alcohol - or Other Drug-Enabled, and Drug-Facilitated Sexual Assault Before and Since Entering CollegeDokumen12 halamanCollege Women's Experiences With Physically Forced, Alcohol - or Other Drug-Enabled, and Drug-Facilitated Sexual Assault Before and Since Entering CollegeGlennKesslerWP100% (1)
- OCPD: Symptoms, Diagnosis and TreatmentDokumen4 halamanOCPD: Symptoms, Diagnosis and TreatmentRana Muhammad Ahmad Khan ManjBelum ada peringkat
- Injeksi Mecobalamin Vas ScoreDokumen5 halamanInjeksi Mecobalamin Vas ScoreHerdy ArshavinBelum ada peringkat
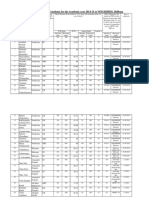
- Admission For 1st Year MBBS Students For The Academic Year 2014-2015Dokumen10 halamanAdmission For 1st Year MBBS Students For The Academic Year 2014-2015Guma KipaBelum ada peringkat
- Chemotherapy-Induced Neuropathic PainDokumen7 halamanChemotherapy-Induced Neuropathic Paintita_leo2Belum ada peringkat
- ICU antibiotic susceptibilities guideDokumen1 halamanICU antibiotic susceptibilities guideFaisal Reza AdiebBelum ada peringkat
- Hubungan Pengetahuan Sikap Penderita Penyakit Malaria FalciparumDokumen63 halamanHubungan Pengetahuan Sikap Penderita Penyakit Malaria FalciparumEsty GulsanBelum ada peringkat
- TMH ResumeDokumen2 halamanTMH Resumeapi-257873078Belum ada peringkat