Anda mungkin juga menyukai
- Nursing Care Plan: Assessment Diagnosis Planning Interventions Rationale EvaluationDokumen11 halamanNursing Care Plan: Assessment Diagnosis Planning Interventions Rationale EvaluationDa NicaBelum ada peringkat
- POST OP BrunnerDokumen7 halamanPOST OP Brunnerjamie carpioBelum ada peringkat
- Doctors OrderDokumen2 halamanDoctors Ordermarc_alvin0% (1)
- Asian Hospital and Medical Center Sample Concept Care Mapping Step 1-5 By: Pamela Mchugh SchusterDokumen3 halamanAsian Hospital and Medical Center Sample Concept Care Mapping Step 1-5 By: Pamela Mchugh SchusterJanelle GimenezBelum ada peringkat
- Nursing Care Plan For Client With Ineffective Tissue PerfusionDokumen2 halamanNursing Care Plan For Client With Ineffective Tissue PerfusionThe Right WayBelum ada peringkat
- Nursing Care Plan StrokeDokumen2 halamanNursing Care Plan StrokeA HBelum ada peringkat
- Unit 6 Part 2 Table - Completed Fall 2023Dokumen2 halamanUnit 6 Part 2 Table - Completed Fall 2023Tanisha SheltonBelum ada peringkat
- NCP PainDokumen5 halamanNCP PainChloe Crystal DorojaBelum ada peringkat
- Urinary Bladder MassDokumen2 halamanUrinary Bladder Masskarl de guzmanBelum ada peringkat
- Algorithms To Guide Your Diagnosis and TreatmentDokumen245 halamanAlgorithms To Guide Your Diagnosis and TreatmentVirgo PotensBelum ada peringkat
- Placenta Previa NCP: Assessment Nursing DX Planning Nursing Inter-Ventions Rationale Expected OutcomeDokumen6 halamanPlacenta Previa NCP: Assessment Nursing DX Planning Nursing Inter-Ventions Rationale Expected OutcomeEugene MananganBelum ada peringkat
- PDF Nursing Care PlanDokumen16 halamanPDF Nursing Care PlanMichael MabiniBelum ada peringkat
- Pneumothorax: Algorithm: Queen's Dect: KGH BleepDokumen2 halamanPneumothorax: Algorithm: Queen's Dect: KGH BleepRachmi Merrina0% (1)
- Readiness For Enhanced Health ManagementDokumen6 halamanReadiness For Enhanced Health ManagementJIMENEZ, TRISHA MARIE D.Belum ada peringkat
- NCP On Postpartum MotherDokumen13 halamanNCP On Postpartum MotherLenjun89% (57)
- Nursing Diagnosis: Risk For Deficient Fluid Volume R/T Traumatic InjuryDokumen2 halamanNursing Diagnosis: Risk For Deficient Fluid Volume R/T Traumatic Injuryarreane yookBelum ada peringkat
- Assessment and Concept Map Care Plan: Elizabeth RouxDokumen6 halamanAssessment and Concept Map Care Plan: Elizabeth Rouxapi-507304905Belum ada peringkat
- Disease & Def Patho/Mech Clinical S/S DX/ Tests/Labs TX NotesDokumen11 halamanDisease & Def Patho/Mech Clinical S/S DX/ Tests/Labs TX NotesSara AshurstBelum ada peringkat
- Peter Hudson Blood TransfusionDokumen29 halamanPeter Hudson Blood TransfusionRyan-Jay AbolenciaBelum ada peringkat
- 2645 Clinical Weekly Worksheet s18Dokumen11 halaman2645 Clinical Weekly Worksheet s18api-502994344Belum ada peringkat
- A Case of Electrical BurnDokumen34 halamanA Case of Electrical BurnryanyganaBelum ada peringkat
- Emergency and Trauma Nursing Study GuideDokumen11 halamanEmergency and Trauma Nursing Study GuideMartha Marty BalintBelum ada peringkat
- Drug Study: Brokenshire CollegeDokumen2 halamanDrug Study: Brokenshire CollegeJai GoBelum ada peringkat
- NCPDokumen3 halamanNCPAlyanna Peñaflorida100% (2)
- Cues Nursing Diagnosis Objectives Interventions Rationale EvaluationDokumen6 halamanCues Nursing Diagnosis Objectives Interventions Rationale EvaluationShereen AlobinayBelum ada peringkat
- Nursing Care Plan: CancerDokumen6 halamanNursing Care Plan: Cancerneuronurse71% (7)
- Drug Study Delivery RoomDokumen7 halamanDrug Study Delivery RoomkhleeoBelum ada peringkat
- NCP (Postpartum Hemmorhage)Dokumen3 halamanNCP (Postpartum Hemmorhage)Anne DyBelum ada peringkat
- NCP HyperthermiaDokumen2 halamanNCP HyperthermiaKirby ContaoiBelum ada peringkat
- Terbutaline SulfateDokumen1 halamanTerbutaline SulfateIvanne Hisoler100% (2)
- Ob GyneDokumen3 halamanOb GynePinky AnchorBelum ada peringkat
- Critical Care NursingDokumen10 halamanCritical Care Nursingianecunar100% (10)
- HeparinDokumen2 halamanHeparinMagdayao Romamea100% (1)
- Angiography (Cardiac Catherization) : Patient Teaching/preparationDokumen2 halamanAngiography (Cardiac Catherization) : Patient Teaching/preparationpsyBelum ada peringkat
- Nursing Care Plan For HELLP SyndromeDokumen17 halamanNursing Care Plan For HELLP SyndromeRosemarie Carpio75% (4)
- Decreased Cardiac Output EclampsiaDokumen6 halamanDecreased Cardiac Output EclampsiaNursesLabs.com100% (7)
- NCPDokumen14 halamanNCPkristapot80% (10)
- Drug StudyDokumen5 halamanDrug StudyJEVEE JEAN BETTERBelum ada peringkat
- Acs - 12.01.2022Dokumen41 halamanAcs - 12.01.2022SabariBelum ada peringkat
- Feline StomatitisDokumen3 halamanFeline StomatitisAntonio SessaBelum ada peringkat
- Rate P Wave QRS Comple X PR Interval: ST RDDokumen2 halamanRate P Wave QRS Comple X PR Interval: ST RDPat G.Belum ada peringkat
- Abdominal PDFDokumen1 halamanAbdominal PDFChakra BaktiBelum ada peringkat
- Pulmonary Edema Concept MapDokumen3 halamanPulmonary Edema Concept MapGeraldine MagnanaoBelum ada peringkat
- 9 - Internal Medicine Buzzwords Handout Oct 2023 John Michael RuizDokumen8 halaman9 - Internal Medicine Buzzwords Handout Oct 2023 John Michael RuizJohn Michael RuizBelum ada peringkat
- Drug StudyDokumen10 halamanDrug StudyFrancis BelotindosBelum ada peringkat
- Hematology: CoagulationDokumen40 halamanHematology: CoagulationMuhammad SaeedBelum ada peringkat
- Concept MapDokumen14 halamanConcept Mapapi-419091662Belum ada peringkat
- نسخة vaginal delieveryDokumen4 halamanنسخة vaginal delieveryرهف الرفاعيBelum ada peringkat
- Ineffective Breathing Pattern Related To Shortness of Breath Possible Evidence by CuesDokumen7 halamanIneffective Breathing Pattern Related To Shortness of Breath Possible Evidence by CuesLouie ParillaBelum ada peringkat
- Test/Treatment What Is It? Complications To Monitor For Nursing Care NotesDokumen5 halamanTest/Treatment What Is It? Complications To Monitor For Nursing Care NotesNieka WBelum ada peringkat
- Nursing Care Plan: Pulmonary EbolismDokumen5 halamanNursing Care Plan: Pulmonary EbolismneuronurseBelum ada peringkat
- Waiters Postpartal Hemorrhage PDFDokumen1 halamanWaiters Postpartal Hemorrhage PDFmp1757Belum ada peringkat
- Nursing of The Childbearing FamilyDokumen3 halamanNursing of The Childbearing Familyroby sorianoBelum ada peringkat
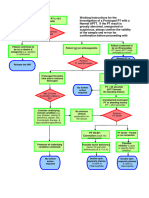
- Working Instructions Investigation of Prolonged PTDokumen1 halamanWorking Instructions Investigation of Prolonged PTtadeariba1Belum ada peringkat
- Epistaxis - Outpatient ManagementDokumen6 halamanEpistaxis - Outpatient ManagementMichael TakariaBelum ada peringkat
- Handling Difficult Patient BehaviorsDokumen4 halamanHandling Difficult Patient BehaviorsneuronurseBelum ada peringkat
- Med Calc: Measurement SystemsDokumen5 halamanMed Calc: Measurement Systemsneuronurse100% (1)
- Enteral Tube FeedingDokumen9 halamanEnteral Tube FeedingneuronurseBelum ada peringkat
- Cultural Sensitivit Y: A Guidebook For Physicians & Healthcare ProfessionalsDokumen30 halamanCultural Sensitivit Y: A Guidebook For Physicians & Healthcare ProfessionalsneuronurseBelum ada peringkat
- Alzheimer Training ManualDokumen73 halamanAlzheimer Training ManualneuronurseBelum ada peringkat
- Calculating Dosages Using Weight MeasurementDokumen3 halamanCalculating Dosages Using Weight MeasurementneuronurseBelum ada peringkat
- Crisis ManagementDokumen8 halamanCrisis ManagementneuronurseBelum ada peringkat
- Linda M. Gorman,: RN, MN, CS, Ocn, CHPNDokumen32 halamanLinda M. Gorman,: RN, MN, CS, Ocn, CHPNneuronurseBelum ada peringkat
- Med Calc: Using Ratio and PorportionDokumen4 halamanMed Calc: Using Ratio and PorportionneuronurseBelum ada peringkat
- Nursing Care Plan: CancerDokumen6 halamanNursing Care Plan: Cancerneuronurse71% (7)
- ECG Learning CenterDokumen377 halamanECG Learning CenterneuronurseBelum ada peringkat
- B - Quick Access Table - Definitions To Abbreviations 1Dokumen21 halamanB - Quick Access Table - Definitions To Abbreviations 1neuronurseBelum ada peringkat
- E-Z ECG Rhythm InterpretationDokumen33 halamanE-Z ECG Rhythm InterpretationneuronurseBelum ada peringkat
- Clinical Applications of Nursing DiagnosisDokumen75 halamanClinical Applications of Nursing DiagnosisneuronurseBelum ada peringkat
- C - Quick Access Table - Combining Forms To Definitions 1Dokumen19 halamanC - Quick Access Table - Combining Forms To Definitions 1neuronurseBelum ada peringkat
- Homeless Care PlanDokumen3 halamanHomeless Care PlanneuronurseBelum ada peringkat
- The Nurse-Client Relationship: Michael Brody, RN, BSNDokumen22 halamanThe Nurse-Client Relationship: Michael Brody, RN, BSNneuronurse100% (1)
- H - Quick Access Table For Suffixes - Definition To Suffix 1Dokumen7 halamanH - Quick Access Table For Suffixes - Definition To Suffix 1neuronurseBelum ada peringkat
- G - Quick Access Table For Suffixes - Suffix To Definition 1Dokumen7 halamanG - Quick Access Table For Suffixes - Suffix To Definition 1neuronurseBelum ada peringkat
- Newborn Nursing Care Plan With ReferncesDokumen6 halamanNewborn Nursing Care Plan With Referncesneuronurse92% (63)
- Nursing Care Plan: Chronic Pain and COPDDokumen11 halamanNursing Care Plan: Chronic Pain and COPDneuronurse100% (1)
- Medical MnemonicsDokumen256 halamanMedical MnemonicssitalcoolkBelum ada peringkat
- Nursing Care Plan: COPDDokumen9 halamanNursing Care Plan: COPDneuronurse88% (32)
- Nursing Care Plan: Pulmonary EbolismDokumen5 halamanNursing Care Plan: Pulmonary EbolismneuronurseBelum ada peringkat
- The Five Rights!: Pedi Atric Skills Lab Administration of Injectable MedicationsDokumen13 halamanThe Five Rights!: Pedi Atric Skills Lab Administration of Injectable Medicationsneuronurse100% (1)
- Lutheran Medical Center Peds Clinical ReferenceDokumen37 halamanLutheran Medical Center Peds Clinical ReferenceneuronurseBelum ada peringkat
- Sleep DeprivationDokumen25 halamanSleep Deprivationdefaagri50% (4)
- Overcoming ShynessDokumen8 halamanOvercoming ShynessLeah OlmosBelum ada peringkat
- Anatomy Helpers Blood Supply To Abdominal OrgansDokumen5 halamanAnatomy Helpers Blood Supply To Abdominal OrgansSam TagardaBelum ada peringkat
- Lab Technologist-2Dokumen32 halamanLab Technologist-2AHAMED SHIFAANBelum ada peringkat
- Plant Structure and Function - Learner's GuideDokumen47 halamanPlant Structure and Function - Learner's Guidehasbiallah1306Belum ada peringkat
- NCP Breast CADokumen3 halamanNCP Breast CAreeyahjonna100% (8)
- TreinsDokumen23 halamanTreinsKosygin LeishangthemBelum ada peringkat
- Chronic Glomerulonephritis in DetailDokumen9 halamanChronic Glomerulonephritis in Detailfile fileBelum ada peringkat
- Xingyi Classics 1.0: Yang Secretly Combine - This Is The Source of XingyiDokumen25 halamanXingyi Classics 1.0: Yang Secretly Combine - This Is The Source of Xingyidionysia100% (13)
- Basic Principles - Snake (First Aid)Dokumen2 halamanBasic Principles - Snake (First Aid)cinnamorollpuffBelum ada peringkat
- Lizard Brain-Bird Brain-Rabbit Brain-Comparative Anatomy - BiozoomDokumen6 halamanLizard Brain-Bird Brain-Rabbit Brain-Comparative Anatomy - BiozoomRuksanurBelum ada peringkat
- ETD-DefibDokumen58 halamanETD-DefibFarah Najwa GhazaliBelum ada peringkat
- The Wound CareDokumen51 halamanThe Wound CareIosefina DudeanuBelum ada peringkat
- IGCSE - Bio - Lesson Plan 6 - CoordinationDokumen3 halamanIGCSE - Bio - Lesson Plan 6 - CoordinationHisokagen100% (2)
- Mode of Action: InsulinDokumen8 halamanMode of Action: Insulinmanus7777100% (1)
- Ubo RampeDokumen332 halamanUbo Rampeberliana syifaBelum ada peringkat
- Singh Et Al. 2022 - PCA - DescriptionDokumen14 halamanSingh Et Al. 2022 - PCA - DescriptionFernanda SantosBelum ada peringkat
- Closed Fractures of The Tibial Diaphysis: David L. Rothberg, MD Erik N. Kubiak, MDDokumen64 halamanClosed Fractures of The Tibial Diaphysis: David L. Rothberg, MD Erik N. Kubiak, MDtilahunthmBelum ada peringkat
- Science of The BreathDokumen71 halamanScience of The BreathRadu GyrBelum ada peringkat
- 2020 08 10 Sanjay Pandarbale Yogesh Nerkar Sufala MalnekarDokumen4 halaman2020 08 10 Sanjay Pandarbale Yogesh Nerkar Sufala MalnekarYogesh NerkarBelum ada peringkat
- CNS Infiltration of Peripheral Immune Cells - D-Day For Neurodegenerative DiseaseDokumen14 halamanCNS Infiltration of Peripheral Immune Cells - D-Day For Neurodegenerative DiseaseFrancesca GrassivaroBelum ada peringkat
- SSC Biology Preivious QuestionsDokumen40 halamanSSC Biology Preivious QuestionsPrabhakar ReddyBelum ada peringkat
- 19.3.2 KidneyDokumen77 halaman19.3.2 KidneyDak AnneBelum ada peringkat
- Physiological Changes in Geriatric PatientsDokumen10 halamanPhysiological Changes in Geriatric Patientsdevwart.caBelum ada peringkat
- 17 Meiosis-SDokumen8 halaman17 Meiosis-Sapi-241253846100% (1)
- Bodybuilding Small File SizeDokumen32 halamanBodybuilding Small File SizeThế Vỹ100% (4)
- Medical Entrance AIPMT PapersDokumen15 halamanMedical Entrance AIPMT Paperssumit kumar0% (1)
- Automated Blood Coagulation Analyzer CA-50: Basic Data Sheet - (Fibrinogen)Dokumen8 halamanAutomated Blood Coagulation Analyzer CA-50: Basic Data Sheet - (Fibrinogen)Aahsan Iqbal احسن اقبالBelum ada peringkat
- Revision Notes CH 3 Human Strengths and Meeting Life ChallengesDokumen8 halamanRevision Notes CH 3 Human Strengths and Meeting Life ChallengesFuljhuri BasuBelum ada peringkat
- Philips Heartstart XL Plus Defibrillator ManualDokumen235 halamanPhilips Heartstart XL Plus Defibrillator ManualvikasBelum ada peringkat