Anda mungkin juga menyukai
- Impaired Physical MobilityDokumen1 halamanImpaired Physical Mobilitykyaw100% (1)
- Pssi 5Dokumen3 halamanPssi 5fuckyouscribd2013041Belum ada peringkat
- Gorean Treatments and ServesDokumen3 halamanGorean Treatments and ServesNishaNightFireBelum ada peringkat
- (New Procedures in Spinal Interventional Neuroradiology) Luigi Manfrà (Eds.) - Spinal Canal Stenosis-Springer International PublisDokumen98 halaman(New Procedures in Spinal Interventional Neuroradiology) Luigi Manfrà (Eds.) - Spinal Canal Stenosis-Springer International PublisThuyet Nguyen PhuocBelum ada peringkat
- 04 CataractsurgeryDokumen16 halaman04 Cataractsurgeryapi-3695929Belum ada peringkat
- Cataract: By: Charmagne MaranonDokumen28 halamanCataract: By: Charmagne MaranonCham'cham Araneta MarañonBelum ada peringkat
- Ears, Eyes, Nose & ThroatDokumen132 halamanEars, Eyes, Nose & ThroatMarnelli_Iris__4261Belum ada peringkat
- Dr. Ashraf Sayeed: Department of OphthalmologyDokumen49 halamanDr. Ashraf Sayeed: Department of Ophthalmologysaiful haque100% (1)
- Care of The Clients With Eye and Ear DisorderDokumen35 halamanCare of The Clients With Eye and Ear DisorderKristine Joy RevañoBelum ada peringkat
- L6 Refractive Errors and PaedsDokumen37 halamanL6 Refractive Errors and PaedsSofíaGriggsBelum ada peringkat
- InggrisDokumen32 halamanInggrisRani Dwi HapsariBelum ada peringkat
- Cataract InformationDokumen25 halamanCataract Informationvasanth_1515Belum ada peringkat
- Chapter 11 Eye & Vision DisordersDokumen72 halamanChapter 11 Eye & Vision DisordersMYLENE GRACE ELARCOSABelum ada peringkat
- Refractive ErrorsDokumen33 halamanRefractive ErrorsMathew Sebastian100% (2)
- Cataract InformationDokumen25 halamanCataract InformationDr.K.M. AbdullaBelum ada peringkat
- CataractsDokumen7 halamanCataractsOktovia KakaBelum ada peringkat
- Opthalmology CasesDokumen10 halamanOpthalmology CasesAhmad SobihBelum ada peringkat
- HYPERMETROPIA and Myopia PDFDokumen55 halamanHYPERMETROPIA and Myopia PDFDrashti ChudasamaBelum ada peringkat
- Concomitant Squint: Noor Asmah MD Azmi Optometrist HsahDokumen56 halamanConcomitant Squint: Noor Asmah MD Azmi Optometrist HsahAnonymous l2Fve4PpD33% (3)
- Ophthalmology Clerks: Alea, Denz Marc Custodio, Audreyfil Perez, Francis MiguelDokumen14 halamanOphthalmology Clerks: Alea, Denz Marc Custodio, Audreyfil Perez, Francis MiguelDenz Marc AleaBelum ada peringkat
- Common Eye Diseases 2022Dokumen33 halamanCommon Eye Diseases 2022Shia LevyBelum ada peringkat
- Eye Disorders: Presented by Carmelita Ramos, RNDokumen65 halamanEye Disorders: Presented by Carmelita Ramos, RNJayme_Galang_7078100% (1)
- CATARACT Case Senario No.1 (Tapel, Joyce T. - BSN3-E)Dokumen4 halamanCATARACT Case Senario No.1 (Tapel, Joyce T. - BSN3-E)SIJIBelum ada peringkat
- Refractive Disorders Blok VisualDokumen27 halamanRefractive Disorders Blok Visualmuhammad ajiBelum ada peringkat
- Visual ProblemsDokumen151 halamanVisual Problemskatrina_rn09Belum ada peringkat
- Cataract SenilisDokumen54 halamanCataract Senilismayo djitroBelum ada peringkat
- CataractDokumen5 halamanCataractAbhinandan SharmaBelum ada peringkat
- Glaucoma and CataractDokumen30 halamanGlaucoma and CataractJayselle ArvieBelum ada peringkat
- Cataract Surgery - : After The ProcedureDokumen16 halamanCataract Surgery - : After The ProcedureAmandeep Singh GandhiBelum ada peringkat
- Eye DisordersDokumen7 halamanEye DisordersClara De GuzmanBelum ada peringkat
- CataractsDokumen21 halamanCataractsRobert L G MabongaBelum ada peringkat
- AMETROPIADokumen48 halamanAMETROPIARahul KirkBelum ada peringkat
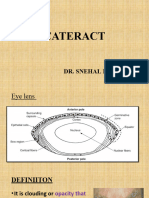
- 1 CataractDokumen31 halaman1 CataractsnehalBelum ada peringkat
- Cataract: Done by Mo3taz Abu Rabiah A7mad LubaniDokumen46 halamanCataract: Done by Mo3taz Abu Rabiah A7mad LubaniMaxwell C Jay KafwaniBelum ada peringkat
- ENUCLEATIONDokumen3 halamanENUCLEATIONTessa BingaroBelum ada peringkat
- Cataract: Done by Jony MallikDokumen46 halamanCataract: Done by Jony MallikAlfa Suryani ArdliBelum ada peringkat
- A Child Presenting With Visual Impairment 28/4/2020Dokumen40 halamanA Child Presenting With Visual Impairment 28/4/2020Sindhu BabuBelum ada peringkat
- Advance Trends in Eye Care: DR Divya Kesarwani Consultant Cataract and Glaucoma ServicesDokumen42 halamanAdvance Trends in Eye Care: DR Divya Kesarwani Consultant Cataract and Glaucoma ServicesdrdivyakesarwaniBelum ada peringkat
- USHM"REZONANCA"FAKULTETI I MJEKËSISË PRISHTINË/Halil AJVAZI/ReSTOR Patient Power Point/Ushtrimet..Dokumen23 halamanUSHM"REZONANCA"FAKULTETI I MJEKËSISË PRISHTINË/Halil AJVAZI/ReSTOR Patient Power Point/Ushtrimet..HALIL Z.AJVAZI100% (1)
- Lecture 11 Special Senses Part 6-VisionDokumen48 halamanLecture 11 Special Senses Part 6-VisionMoses Jr KazevuBelum ada peringkat
- Presented by Carmelita Ramos, RNDokumen81 halamanPresented by Carmelita Ramos, RNMela De Jesus RamosBelum ada peringkat
- Extracapsular Cataract Extraction (OR)Dokumen4 halamanExtracapsular Cataract Extraction (OR)Jet-Jet GuillerganBelum ada peringkat
- CataractsDokumen37 halamanCataractsIbrahimalpha BadarakamaraBelum ada peringkat
- Lay Forum NotesDokumen7 halamanLay Forum NotesCleoGomezBelum ada peringkat
- MonovisionDokumen3 halamanMonovisionenglish-exactlyBelum ada peringkat
- AstigmatismDokumen18 halamanAstigmatismAmie CuevasBelum ada peringkat
- CataractsDokumen47 halamanCataractsNrs Sani Sule MashiBelum ada peringkat
- 1 - MyopiaDokumen9 halaman1 - MyopiaSpislgal PhilipBelum ada peringkat
- Eyecare Review - : For Primary Care PractitionersDokumen108 halamanEyecare Review - : For Primary Care PractitionersprilaviaramadhaniBelum ada peringkat
- MR Cresswell Final PresentationDokumen11 halamanMR Cresswell Final PresentationFIRUZ YUMULBelum ada peringkat
- Cataract JemDokumen17 halamanCataract JemJemsMei Comparativo MensuradoBelum ada peringkat
- Cataract: Mohd Roslee Bin Abd GhaniDokumen46 halamanCataract: Mohd Roslee Bin Abd GhaniSaha DirllahBelum ada peringkat
- Myopia or Nearsightedness: A Refractive Error of The EyeDokumen9 halamanMyopia or Nearsightedness: A Refractive Error of The EyeClaire LimosBelum ada peringkat
- Cataract Information For Patients: and Click On Wait Times TabDokumen13 halamanCataract Information For Patients: and Click On Wait Times TabVidini Kusuma AjiBelum ada peringkat
- Optics and Refraction For 5 Year Medical Students Mutaz Gharaibeh, MDDokumen52 halamanOptics and Refraction For 5 Year Medical Students Mutaz Gharaibeh, MDShahar ShababBelum ada peringkat
- Retinal DetachmentDokumen19 halamanRetinal DetachmentJohn Hans CaturasBelum ada peringkat
- Ocular Terminology in Primary Eye Care: Susan A. Resni CK, O.D. FAAO, FSLS New Yor K, NYDokumen46 halamanOcular Terminology in Primary Eye Care: Susan A. Resni CK, O.D. FAAO, FSLS New Yor K, NYahmad weqarBelum ada peringkat
- D-L Cataract Information JVC - PPSDokumen25 halamanD-L Cataract Information JVC - PPSDr Kirti ChhapiaBelum ada peringkat
- Activity5 (Retinal Detachment)Dokumen3 halamanActivity5 (Retinal Detachment)Gabbii CincoBelum ada peringkat
- Sensation: Hearing, Vision, Taste, Touch, and SmellDokumen99 halamanSensation: Hearing, Vision, Taste, Touch, and SmellMichelle LindsayBelum ada peringkat
- Cataract Service - 1Dokumen11 halamanCataract Service - 1sanjuBelum ada peringkat
- Retina Detachment, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionDari EverandRetina Detachment, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionBelum ada peringkat
- Low Vision: Assessment and Educational Needs: A Guide to Teachers and ParentsDari EverandLow Vision: Assessment and Educational Needs: A Guide to Teachers and ParentsBelum ada peringkat
- Visual Field Loss in the Real World: A Book of Static Perimetry Test Targets for Eye Health ProfessionalsDari EverandVisual Field Loss in the Real World: A Book of Static Perimetry Test Targets for Eye Health ProfessionalsBelum ada peringkat
- Skin Disorders 4-2-08Dokumen14 halamanSkin Disorders 4-2-08api-3822433Belum ada peringkat
- EarDokumen7 halamanEarapi-3822433Belum ada peringkat
- OsteoporosisDokumen3 halamanOsteoporosisapi-3822433Belum ada peringkat
- OsteoarthritisDokumen2 halamanOsteoarthritisapi-3822433Belum ada peringkat
- Emergency Care 3-27-08Dokumen14 halamanEmergency Care 3-27-08api-3822433Belum ada peringkat
- Carpal Tunnel SyndromeDokumen2 halamanCarpal Tunnel Syndromeapi-3822433Belum ada peringkat
- GoutDokumen2 halamanGoutapi-3822433Belum ada peringkat
- EyesDokumen4 halamanEyesapi-3822433Belum ada peringkat
- Eating Disorders 2-13-08Dokumen8 halamanEating Disorders 2-13-08api-3822433Belum ada peringkat
- Legal 2-13-08Dokumen3 halamanLegal 2-13-08api-3822433Belum ada peringkat
- Schizophrenia 2-06-07Dokumen2 halamanSchizophrenia 2-06-07api-3822433Belum ada peringkat
- Burns 3-26-08Dokumen15 halamanBurns 3-26-08api-3822433Belum ada peringkat
- DepressionDokumen4 halamanDepressionapi-3822433Belum ada peringkat
- Disorders of Children and AdolescentsDokumen17 halamanDisorders of Children and Adolescentsapi-3822433Belum ada peringkat
- Alt. Communication/ Motor FunctionDokumen11 halamanAlt. Communication/ Motor Functionapi-3822433Belum ada peringkat
- Altered LOC and Increased ICP 1-16-07Dokumen15 halamanAltered LOC and Increased ICP 1-16-07api-3822433Belum ada peringkat
- Tca 5 1-30-08Dokumen8 halamanTca 5 1-30-08api-3822433Belum ada peringkat
- Crisis 2-08-07Dokumen9 halamanCrisis 2-08-07api-3822433Belum ada peringkat
- Tramatic Brain Injury 1-24-08Dokumen9 halamanTramatic Brain Injury 1-24-08api-3822433Belum ada peringkat
- Tca 3 1-23-07Dokumen14 halamanTca 3 1-23-07api-3822433Belum ada peringkat
- Concepts and IssuesDokumen8 halamanConcepts and Issuesapi-3822433Belum ada peringkat
- Organizational ManagementDokumen5 halamanOrganizational Managementapi-3822433Belum ada peringkat
- Nursing in DisastersDokumen18 halamanNursing in Disastersapi-3822433Belum ada peringkat
- Traction 3-05-08Dokumen6 halamanTraction 3-05-08api-3822433Belum ada peringkat
- TCA 3 Amputation 2-29-08Dokumen9 halamanTCA 3 Amputation 2-29-08api-3822433Belum ada peringkat
- Legal Ethical 4-24-08Dokumen16 halamanLegal Ethical 4-24-08api-3822433Belum ada peringkat
- TCA 3 Osteomyelitis 2-29-08Dokumen6 halamanTCA 3 Osteomyelitis 2-29-08api-3822433Belum ada peringkat
- Tca 5 Ra, Sle 3-06-08Dokumen6 halamanTca 5 Ra, Sle 3-06-08api-3822433Belum ada peringkat
- TCA 2 Scoliosis 2-28-08Dokumen18 halamanTCA 2 Scoliosis 2-28-08api-3822433Belum ada peringkat
- Fractures TCA 1 2-27-08Dokumen6 halamanFractures TCA 1 2-27-08api-3822433Belum ada peringkat
- Pre Prosthetic SurgeryDokumen98 halamanPre Prosthetic SurgeryKharismaNisaBelum ada peringkat
- An Experience With Dome Osteotomy. Final Copy (123224)Dokumen8 halamanAn Experience With Dome Osteotomy. Final Copy (123224)Arsalan BukhariBelum ada peringkat
- Triage Level 5Dokumen78 halamanTriage Level 5DanielKnows100% (1)
- Life Vision Upper Intermediate WorkbookDokumen129 halamanLife Vision Upper Intermediate WorkbookGrace FreudBelum ada peringkat
- Morariu DDDprelimASN (1) (Compatibility Mode)Dokumen25 halamanMorariu DDDprelimASN (1) (Compatibility Mode)SAKSHI KATIYARBelum ada peringkat
- The Skeletal System Tarpapel 6Dokumen6 halamanThe Skeletal System Tarpapel 6JONNALYN ALARCONBelum ada peringkat
- Will Fleming Olympic Lifting BookDokumen112 halamanWill Fleming Olympic Lifting Bookrianselve3100% (5)
- TRM 409.01 "Ethics of Consumer Production and Marketing"Dokumen4 halamanTRM 409.01 "Ethics of Consumer Production and Marketing"Neşe RomanBelum ada peringkat
- Lazy Girl WorkoutDokumen17 halamanLazy Girl Workoutسميره محمدBelum ada peringkat
- Burn It All DownDokumen143 halamanBurn It All DownkikiBelum ada peringkat
- Bomba - ITT - Família 3171Dokumen76 halamanBomba - ITT - Família 3171UezilheiBelum ada peringkat
- Perineal HematomDokumen11 halamanPerineal HematomLance TapelBelum ada peringkat
- Patient Care Session 8 Flipped ClassroomDokumen7 halamanPatient Care Session 8 Flipped ClassroomNurliyana Zairul AfendiBelum ada peringkat
- Mouseheart 2: Hopper's Destiny by Lisa Fiedler (Excerpt)Dokumen63 halamanMouseheart 2: Hopper's Destiny by Lisa Fiedler (Excerpt)Simon and Schuster75% (4)
- Phrenic Nerve DamageDokumen15 halamanPhrenic Nerve DamageIzza Mae Ferrancol PastranaBelum ada peringkat
- BIRTH INJURIES FinalDokumen48 halamanBIRTH INJURIES FinalAlvin OmondiBelum ada peringkat
- Kaplan Decision Tree and All Nurses NotesDokumen103 halamanKaplan Decision Tree and All Nurses NotesTravel Junky100% (1)
- Erezo V JepteDokumen3 halamanErezo V JeptePJr Millete0% (1)
- Lesson 2: First Aid Qualities of A Good First Aider: Gentle Observant Resorceful Sympathetic Tactful CheerfulDokumen4 halamanLesson 2: First Aid Qualities of A Good First Aider: Gentle Observant Resorceful Sympathetic Tactful CheerfulDexter BangayanBelum ada peringkat
- Jigy WirgleDokumen486 halamanJigy Wirglesierleinad1Belum ada peringkat
- Health Optimizing Physical Education 1Dokumen17 halamanHealth Optimizing Physical Education 1Niko ChavezBelum ada peringkat
- Color Atlas Minor SurgeryDokumen121 halamanColor Atlas Minor SurgeryRifQi KurniawanBelum ada peringkat
- First Aid Unit PlanDokumen27 halamanFirst Aid Unit Planapi-497283129Belum ada peringkat
- Affidavit Complaint Slight Physical InjuryDokumen2 halamanAffidavit Complaint Slight Physical Injuryduanepo100% (1)
- Casts & Splints WhoDokumen4 halamanCasts & Splints WhodocpanchuBelum ada peringkat
- Basic Workshop Practice TME 121: Dr. David Fadare Mechanical Engineering Department University of IbadanDokumen27 halamanBasic Workshop Practice TME 121: Dr. David Fadare Mechanical Engineering Department University of Ibadandude GFABelum ada peringkat