Anda mungkin juga menyukai
- CIPD Level 5 HR RMT Assessment Brief v1.0Dokumen3 halamanCIPD Level 5 HR RMT Assessment Brief v1.0Khushbu0% (2)
- Prescribing For Self or FamilyDokumen15 halamanPrescribing For Self or Familycarramrod2100% (2)
- Digital Unit Plan - Pride and PrejudiceDokumen5 halamanDigital Unit Plan - Pride and PrejudiceErin Gonzalez50% (2)
- Advocacy Series Module1Dokumen22 halamanAdvocacy Series Module1Abdul Mujeeb KhanBelum ada peringkat
- Diabetes and Hypertension: A Comprehensive Report On Management and The Prevention of Cardiovascular and Renal ComplicationsDokumen3 halamanDiabetes and Hypertension: A Comprehensive Report On Management and The Prevention of Cardiovascular and Renal Complicationsrizqi_cepiBelum ada peringkat
- Diabetes and Cardiovascular DiseaseDokumen119 halamanDiabetes and Cardiovascular DiseaseAlina PopaBelum ada peringkat
- Case HistoryDokumen8 halamanCase HistoryjabeensarwarBelum ada peringkat
- Dia Care-2005-Sever-1151-7Dokumen7 halamanDia Care-2005-Sever-1151-7Barbara Sakura RiawanBelum ada peringkat
- Ban JASH2009Dokumen15 halamanBan JASH2009Adek FahmialdiBelum ada peringkat
- Case Study Hypertension - EditedDokumen8 halamanCase Study Hypertension - EditedJayReneBelum ada peringkat
- JNC 8Dokumen14 halamanJNC 8amiwahyuniBelum ada peringkat
- HTN Guidelines 1Dokumen12 halamanHTN Guidelines 1lakshminivas PingaliBelum ada peringkat
- Benefits and Risks of Antihypertensive Medications in The ElderlyDokumen28 halamanBenefits and Risks of Antihypertensive Medications in The ElderlyNasrull BinHzBelum ada peringkat
- s80 FullDokumen3 halamans80 FullDiego OrtechoBelum ada peringkat
- Accord Trial Update - FinalDokumen3 halamanAccord Trial Update - FinalTyler HoffmanBelum ada peringkat
- Hypertension: A Focus On JNC VIIDokumen95 halamanHypertension: A Focus On JNC VIITri GumilarBelum ada peringkat
- Case Study: Treating Hypertension in Patients With DiabetesDokumen10 halamanCase Study: Treating Hypertension in Patients With Diabetesfirda rydBelum ada peringkat
- AHA/ADA Scientific StatementDokumen29 halamanAHA/ADA Scientific StatementpukpigjBelum ada peringkat
- Tilburg University: Franse, L.V. Pahor, M. Di Bari, M. Somes, G.W. Cushman, W.C. Applegate, W.BDokumen8 halamanTilburg University: Franse, L.V. Pahor, M. Di Bari, M. Somes, G.W. Cushman, W.C. Applegate, W.Bpooria shBelum ada peringkat
- 10 1 1 549 3097Dokumen9 halaman10 1 1 549 3097RISTOBelum ada peringkat
- Hta 8 JNCDokumen14 halamanHta 8 JNCLuis CelyBelum ada peringkat
- JSC 130010Dokumen14 halamanJSC 130010Aqsha AmandaBelum ada peringkat
- 1 s2.0 S0002870320302143 MainDokumen9 halaman1 s2.0 S0002870320302143 MaindeepBelum ada peringkat
- Circulation 2011 Smith 2458 73Dokumen18 halamanCirculation 2011 Smith 2458 73tvmedicineBelum ada peringkat
- Clinical Management of Hypertensive Heart DiseaseDokumen22 halamanClinical Management of Hypertensive Heart DiseaseTrixie Anne GamotinBelum ada peringkat
- Icc UltimoDokumen18 halamanIcc UltimoJoshua Alberto Gracia MancillaBelum ada peringkat
- Cardiovascular Safety Profile of Currently Available Diabetic DrugsDokumen17 halamanCardiovascular Safety Profile of Currently Available Diabetic Drugsvina_nursyaidahBelum ada peringkat
- Hta TtoDokumen13 halamanHta TtoAmelia RiveraBelum ada peringkat
- Case Study: Treating Hypertension in Patients With Diabetes: Presentation CommentaryDokumen9 halamanCase Study: Treating Hypertension in Patients With Diabetes: Presentation CommentaryJohn PauloBelum ada peringkat
- AHA Scientific Statement: Resistant Hypertension: Detection, Evaluation, and ManagementDokumen38 halamanAHA Scientific Statement: Resistant Hypertension: Detection, Evaluation, and ManagementPratik TripathiBelum ada peringkat
- jnc8 PDFDokumen14 halamanjnc8 PDFRizki NovitasariBelum ada peringkat
- Circulation 2012 Berger 491 500Dokumen11 halamanCirculation 2012 Berger 491 500Nurul Azmi Rosmala PutriBelum ada peringkat
- Diabetes and Hypertension: A Comparative Review of Current GuidelinesDokumen6 halamanDiabetes and Hypertension: A Comparative Review of Current GuidelineskartikayuanafitriBelum ada peringkat
- Hypertension (HighBloodPressure) (NHLBI) PDFDokumen2 halamanHypertension (HighBloodPressure) (NHLBI) PDFHarsha Jeevan Kishore KaranamBelum ada peringkat
- Omapatrilat Case Study FullDokumen2 halamanOmapatrilat Case Study FullOladapo AlabedeBelum ada peringkat
- HTA CanadaDokumen3 halamanHTA Canadavasarhely imolaBelum ada peringkat
- Hypertension in People With Type 2 DiabetesDokumen6 halamanHypertension in People With Type 2 DiabetesIgor CampanaBelum ada peringkat
- Out 21 PDFDokumen10 halamanOut 21 PDFBlank SpaceBelum ada peringkat
- Treatment of Hypertension in Adults With Diabetes: Position StatementDokumen3 halamanTreatment of Hypertension in Adults With Diabetes: Position StatementVera WatiBelum ada peringkat
- Diabetic HypertensionDokumen5 halamanDiabetic HypertensionmabrarahmedBelum ada peringkat
- Research Paper On Hypertension PDFDokumen5 halamanResearch Paper On Hypertension PDFaflbqtfvh100% (1)
- Cost Effectiveness and Resource AllocationDokumen7 halamanCost Effectiveness and Resource AllocationSarah AmeliaBelum ada peringkat
- Oral Heart Failure Medications: An Update For Home Health CliniciansDokumen12 halamanOral Heart Failure Medications: An Update For Home Health CliniciansSaraTravassosBelum ada peringkat
- Erectile Dysfunction and HypertensionDokumen8 halamanErectile Dysfunction and HypertensionILham SyahBelum ada peringkat
- Antihypertensive Drug Class Interactions and Risk For Incident Diabetes: A Nested Case - Control StudyDokumen9 halamanAntihypertensive Drug Class Interactions and Risk For Incident Diabetes: A Nested Case - Control StudylalaBelum ada peringkat
- Pi Is 1499267113000373 ObatDokumen3 halamanPi Is 1499267113000373 Obatscd_chesa_189432221Belum ada peringkat
- Research Paper Congestive Heart FailureDokumen6 halamanResearch Paper Congestive Heart Failurelzpyreqhf100% (1)
- JNC 8 SummaryDokumen14 halamanJNC 8 Summaryamm1101Belum ada peringkat
- Pi Is 1933171110000434Dokumen9 halamanPi Is 1933171110000434Jonathan Ian ArinsolBelum ada peringkat
- New England Journal Medicine: The ofDokumen5 halamanNew England Journal Medicine: The ofAri Hidriansyah AtmajaBelum ada peringkat
- Heart Failure and Diabetes Endo Metab Clinics North Am 17Dokumen19 halamanHeart Failure and Diabetes Endo Metab Clinics North Am 17Paulina DiazBelum ada peringkat
- 2015 Article 244Dokumen8 halaman2015 Article 244nasar adenBelum ada peringkat
- Hypertension Thesis StatementDokumen4 halamanHypertension Thesis StatementBuyAPaperOnlineUK100% (2)
- Review JNC 8 PDFDokumen3 halamanReview JNC 8 PDFandirio7486Belum ada peringkat
- Hypoglycemia in Diabetes: Pathophysiology, Prevalence, and PreventionDari EverandHypoglycemia in Diabetes: Pathophysiology, Prevalence, and PreventionBelum ada peringkat
- Sitti Hajijah SooDokumen16 halamanSitti Hajijah SooijahsooBelum ada peringkat
- Research Paper HypertensionDokumen4 halamanResearch Paper Hypertensionfvf66j19100% (1)
- Clinical GuidelineDokumen12 halamanClinical Guidelineazab00Belum ada peringkat
- Lecture 2 HypertensionDokumen32 halamanLecture 2 HypertensionJalil HaddadinBelum ada peringkat
- Meeting the American Diabetes Association Standards of Care: An Algorithmic Approach to Clinical Care of the Diabetes PatientDari EverandMeeting the American Diabetes Association Standards of Care: An Algorithmic Approach to Clinical Care of the Diabetes PatientBelum ada peringkat
- Meeting the American Diabetes Association Standards of CareDari EverandMeeting the American Diabetes Association Standards of CareBelum ada peringkat
- Diabetes Risks from Prescription and Nonprescription Drugs: Mechanisms and Approaches to Risk ReductionDari EverandDiabetes Risks from Prescription and Nonprescription Drugs: Mechanisms and Approaches to Risk ReductionBelum ada peringkat
- Comparison of Common Meds For Diabetic Neuropathy: Pharmacist'S Letter / Prescriber'S LetterDokumen5 halamanComparison of Common Meds For Diabetic Neuropathy: Pharmacist'S Letter / Prescriber'S Lettercarramrod2Belum ada peringkat
- 250803111111Dokumen4 halaman250803111111carramrod2Belum ada peringkat
- 1253Dokumen3 halaman1253carramrod2Belum ada peringkat
- 1215Dokumen11 halaman1215carramrod2Belum ada peringkat
- Selecting A Sulfonylurea: Pharmacist'S Letter / Prescriber'S LetterDokumen3 halamanSelecting A Sulfonylurea: Pharmacist'S Letter / Prescriber'S Lettercarramrod2Belum ada peringkat
- DfsefDokumen4 halamanDfsefcarramrod2Belum ada peringkat
- 1214Dokumen4 halaman1214carramrod2Belum ada peringkat
- Initiation and Adjustment of Insulin Regimens For Type 2 DiabetesDokumen2 halamanInitiation and Adjustment of Insulin Regimens For Type 2 Diabetescarramrod2Belum ada peringkat
- 205rfqergqergDokumen4 halaman205rfqergqergcarramrod2Belum ada peringkat
- 1107Dokumen5 halaman1107carramrod2Belum ada peringkat
- Treatment of Diabetes in Women Who Are Pregnant: Pharmacist'S Letter / Prescriber'S LetterDokumen5 halamanTreatment of Diabetes in Women Who Are Pregnant: Pharmacist'S Letter / Prescriber'S Lettercarramrod2Belum ada peringkat
- Proper Disposal of Expired or Unwanted DrugsDokumen9 halamanProper Disposal of Expired or Unwanted Drugscarramrod2Belum ada peringkat
- 3807Dokumen2 halaman3807carramrod2Belum ada peringkat
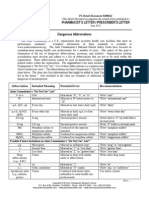
- Dangerous AbbreviationsDokumen3 halamanDangerous Abbreviationscarramrod2Belum ada peringkat
- Tablet Splitting - To Split or Not To SplitDokumen2 halamanTablet Splitting - To Split or Not To Splitcarramrod2Belum ada peringkat
- Management of Common Skin DiseasesDokumen17 halamanManagement of Common Skin Diseasescarramrod2Belum ada peringkat
- Generic Drug VariabilityDokumen5 halamanGeneric Drug Variabilitycarramrod2Belum ada peringkat
- Sample Interview Questions - BridgespanDokumen5 halamanSample Interview Questions - BridgespanMukesh JakharBelum ada peringkat
- Formulation Optimization of A Palm-Based Nanoemulsion System Containing LevodopaDokumen16 halamanFormulation Optimization of A Palm-Based Nanoemulsion System Containing LevodopaAnton MelcherBelum ada peringkat
- Analyzing The Effectiveness of Reward Management System On Employee Performance Through The Mediating Role of Employee MotivationDokumen12 halamanAnalyzing The Effectiveness of Reward Management System On Employee Performance Through The Mediating Role of Employee MotivationRenz Dela Cruz ArellanoBelum ada peringkat
- Brain Training WorkDokumen84 halamanBrain Training WorkTao CmBelum ada peringkat
- BLD-Know Your Planet Grade 5Dokumen8 halamanBLD-Know Your Planet Grade 5Anu ReddyBelum ada peringkat
- Sun2019 PDFDokumen10 halamanSun2019 PDFCristinaBelum ada peringkat
- 485Dokumen80 halaman485Bqdcc6Belum ada peringkat
- CB Chapter 11 Group Influence and Social Media Sixth EditionDokumen16 halamanCB Chapter 11 Group Influence and Social Media Sixth EditionMike CloryBelum ada peringkat
- Clinically Proven Herbal Toothpaste in Sri LankaDokumen7 halamanClinically Proven Herbal Toothpaste in Sri LankaYoga ChanBelum ada peringkat
- Detailed Urban Land Use Land Cover ClassificationDokumen24 halamanDetailed Urban Land Use Land Cover ClassificationZaman RaiBelum ada peringkat
- Leadership Skill Leadership Skill: Lecture by Affifa Sardar Lecture by Affifa SardarDokumen42 halamanLeadership Skill Leadership Skill: Lecture by Affifa Sardar Lecture by Affifa SardarmeaowBelum ada peringkat
- Transportation Economics and Project AppraisalDokumen3 halamanTransportation Economics and Project Appraisalharish babu aluruBelum ada peringkat
- Jadwal NEAT SG 1Dokumen5 halamanJadwal NEAT SG 1sangkertadiBelum ada peringkat
- Thesis Summary OutlineDokumen4 halamanThesis Summary Outlinekatiegulleylittlerock100% (2)
- Researching and Writing A Dissertation An Essential Guide For Business Students PDFDokumen8 halamanResearching and Writing A Dissertation An Essential Guide For Business Students PDFPaperHelperUKBelum ada peringkat
- A8 Maersk CaseDokumen5 halamanA8 Maersk CaseSuduBelum ada peringkat
- Chapter 3 PerceptionDokumen21 halamanChapter 3 PerceptionMuhd AshrafBelum ada peringkat
- Sales and Distribution Management: Project ReportDokumen58 halamanSales and Distribution Management: Project ReportKaran ShahBelum ada peringkat
- Board Structure As DeterminantDokumen11 halamanBoard Structure As DeterminantJamil LagiBelum ada peringkat
- Mining-Calculator ProjectExample PDFDokumen46 halamanMining-Calculator ProjectExample PDFwalterloliBelum ada peringkat
- Master Thesis in LiteratureDokumen5 halamanMaster Thesis in Literaturegja8e2sv100% (2)
- PecinovaLostakovaHavranek KVDokumen7 halamanPecinovaLostakovaHavranek KVNina NugraBelum ada peringkat
- Global Perspectives PaperDokumen9 halamanGlobal Perspectives Paperapi-373229634Belum ada peringkat
- Nurse's Practice Concerning Mouth Care For Unconscious or Debilitated PatientDokumen5 halamanNurse's Practice Concerning Mouth Care For Unconscious or Debilitated PatientFikri IramaBelum ada peringkat
- BenchmarkingDokumen14 halamanBenchmarkingNarnish100% (1)
- Systematic Literature Review: Kemampuan Pembuktian MatematisDokumen15 halamanSystematic Literature Review: Kemampuan Pembuktian MatematisAdam SIBelum ada peringkat
- Forgiveness, Personality and Gratitude: Short CommunicationDokumen11 halamanForgiveness, Personality and Gratitude: Short CommunicationOana MariaBelum ada peringkat