Anda mungkin juga menyukai
- Video Epilepsi: Epileptic Fit (Epileptický Záchvat) .WMVDokumen59 halamanVideo Epilepsi: Epileptic Fit (Epileptický Záchvat) .WMVYudia MahardikaBelum ada peringkat
- Chest Pain NICEDokumen52 halamanChest Pain NICEAliya Batrisya AliyaBelum ada peringkat
- Hepatitis FulminanDokumen5 halamanHepatitis FulminanAliya Batrisya AliyaBelum ada peringkat
- 18 UrolithiasisDokumen104 halaman18 UrolithiasisJuliana AlzateBelum ada peringkat
- Surgical NotesDokumen3 halamanSurgical NotesAliya Batrisya AliyaBelum ada peringkat
- Embryonic Period: by DR Daw Khin WinDokumen40 halamanEmbryonic Period: by DR Daw Khin WinAliya Batrisya AliyaBelum ada peringkat
- SIGN Management PSMBADokumen64 halamanSIGN Management PSMBAAliya Batrisya AliyaBelum ada peringkat
- Psychiatry and EthicsDokumen53 halamanPsychiatry and EthicsnoviceboyBelum ada peringkat
- SimpsFoMed 12thenDokumen209 halamanSimpsFoMed 12thenAliya Batrisya Aliya100% (1)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Blood Flow Mechanics in Cardiovascular DevelopmentDokumen15 halamanBlood Flow Mechanics in Cardiovascular Developmentromane gaston bretonBelum ada peringkat
- Physical Assessment of Cardiovascular SystemDokumen31 halamanPhysical Assessment of Cardiovascular SystemaagBelum ada peringkat
- An - Sci 1 Intro To Animals Science 2Dokumen98 halamanAn - Sci 1 Intro To Animals Science 2Ramil Jr. EntanaBelum ada peringkat
- Admission Inferior Vena Cava Measurements Are Associated With Mortality After Hospitalization For Acute Decompensated Heart FailureDokumen18 halamanAdmission Inferior Vena Cava Measurements Are Associated With Mortality After Hospitalization For Acute Decompensated Heart FailurePuja Nastia LubisBelum ada peringkat
- European J of Heart Fail - 2017 - Gorter - Right Heart Dysfunction and Failure in Heart Failure With Preserved EjectionDokumen22 halamanEuropean J of Heart Fail - 2017 - Gorter - Right Heart Dysfunction and Failure in Heart Failure With Preserved EjectionAlexandru MartBelum ada peringkat
- (Mahesh Chandra) Objective Cardiology PDFDokumen609 halaman(Mahesh Chandra) Objective Cardiology PDFfajarBelum ada peringkat
- Manual T12 Patient Montior User ManualDokumen93 halamanManual T12 Patient Montior User ManualzorgglubBelum ada peringkat
- Animal Science 121 Principles To Animal Science Compiled by Dr. Erwin L. IcallaDokumen19 halamanAnimal Science 121 Principles To Animal Science Compiled by Dr. Erwin L. IcallaJamielyne Rizza AtienzaBelum ada peringkat
- f2 Biology Simplified Notes SPDokumen30 halamanf2 Biology Simplified Notes SPmicah isaboke100% (2)
- Cardiac Cycle: DR Rakesh JainDokumen97 halamanCardiac Cycle: DR Rakesh JainKemoy FrancisBelum ada peringkat
- Pacemaker Learning Package: Paula Nekic CNE Liverpool Hospital ICU January 2016Dokumen46 halamanPacemaker Learning Package: Paula Nekic CNE Liverpool Hospital ICU January 2016Zahangir Kabir AshikBelum ada peringkat
- Specifications For SSI-8000 High-Performance Color SystemDokumen19 halamanSpecifications For SSI-8000 High-Performance Color SystemMedLab Şamaxı KlinikasıBelum ada peringkat
- Cardiac Cycle of The Heart PPT 3Dokumen18 halamanCardiac Cycle of The Heart PPT 3pshantanu123Belum ada peringkat
- Heart FailureDokumen29 halamanHeart Failuremerin sunilBelum ada peringkat
- Cardiac CycleDokumen3 halamanCardiac CycleNorazlina MnBelum ada peringkat
- The Diagram Shows A Section Through The Heart of A MammalDokumen36 halamanThe Diagram Shows A Section Through The Heart of A Mammaldaisuke ʕ•ᴥ•ʔBelum ada peringkat
- Pathophysiology of HCVDDokumen5 halamanPathophysiology of HCVDNicolne Lorraine100% (1)
- Patofisologi Gagal JantungDokumen38 halamanPatofisologi Gagal JantungRizqy JoeandriBelum ada peringkat
- Arc PDFDokumen549 halamanArc PDFSneha BaldotaBelum ada peringkat
- Cardiac Physical ExamDokumen45 halamanCardiac Physical ExamARIANNE JOY TAMARAY100% (1)
- 04-The Cardiac Cycle - Wigger's Diagram (J Swanevelder)Dokumen6 halaman04-The Cardiac Cycle - Wigger's Diagram (J Swanevelder)Patrick WilliamsBelum ada peringkat
- Cardiac Cycle JVPDokumen70 halamanCardiac Cycle JVPAstrid PramudyaaBelum ada peringkat
- VT Bradycardias AnswDokumen128 halamanVT Bradycardias AnswJoshua-Majid ShahbaziBelum ada peringkat
- Template EchoreportDokumen1 halamanTemplate EchoreportArijitArikNath100% (1)
- Atrial Cardiomypathy 2023 FrontiersDokumen11 halamanAtrial Cardiomypathy 2023 FrontiersAxel Hiram Hernandez PinedaBelum ada peringkat
- Cardiovascular SystemDokumen6 halamanCardiovascular Systemtasneem8Belum ada peringkat
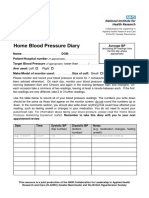
- Home Blood Pressure DiaryDokumen2 halamanHome Blood Pressure DiaryCherieBelum ada peringkat
- Echocardiogrphy Instrumentasi and Color Doppler. 2023 Ir CahyoDokumen90 halamanEchocardiogrphy Instrumentasi and Color Doppler. 2023 Ir CahyoJalu PanjongkoBelum ada peringkat
- Elementary First Aid Power Point (Efa) - oRIGINALDokumen183 halamanElementary First Aid Power Point (Efa) - oRIGINALClark Llamera100% (1)
- Lorma Colleges College of Physical and Respiratory TherapyDokumen33 halamanLorma Colleges College of Physical and Respiratory TherapyAnab Mohamed Elhassan Abbas AlnowBelum ada peringkat