Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (894)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
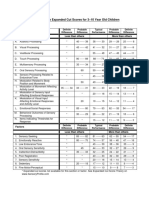
- Sensory Profile Expanded Cut Scores For 3-10 Year Old ChildrenDokumen1 halamanSensory Profile Expanded Cut Scores For 3-10 Year Old ChildrenAyra MagpiliBelum ada peringkat
- Khilafat o Malookeyat Syed Abul Ala Maududi UrduDokumen336 halamanKhilafat o Malookeyat Syed Abul Ala Maududi Urdujawwad ahmed khan82% (51)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Treatment Resistance in Psychiatry - Risk Factors, Biology, and Management-Springer Singapore (2019) PDFDokumen415 halamanTreatment Resistance in Psychiatry - Risk Factors, Biology, and Management-Springer Singapore (2019) PDFDrAvik Chakraborty100% (1)
- Brown PDFDokumen20 halamanBrown PDFccareemail100% (1)
- Kalam e IqbalDokumen14 halamanKalam e Iqbalapi-19502000Belum ada peringkat
- Detecting The Differences Radiculopathy, Myelopathy and Peripheral NeuropathyDokumen70 halamanDetecting The Differences Radiculopathy, Myelopathy and Peripheral Neuropathyapi-19502000100% (8)
- Brain Death Anatomy and PhysiologyDokumen66 halamanBrain Death Anatomy and Physiologyapi-19502000Belum ada peringkat
- Brain Tumour Presentation AftabDokumen56 halamanBrain Tumour Presentation Aftabapi-19502000Belum ada peringkat
- Cervical Spine InjuryDokumen64 halamanCervical Spine Injuryapi-195020000% (1)
- Neuroanatomy Practical 2nd ShiftDokumen2 halamanNeuroanatomy Practical 2nd Shiftapi-19502000Belum ada peringkat
- Acute Low Back Pain - Zafa - Iqbal - DRDokumen69 halamanAcute Low Back Pain - Zafa - Iqbal - DRapi-19502000Belum ada peringkat
- Pineal Meningiomas3Dokumen1 halamanPineal Meningiomas3api-19502000Belum ada peringkat
- NerosurgeryDokumen34 halamanNerosurgeryapi-19502000100% (1)
- Results of Various Modalities of Treatment For Acute Subdural Hematomas in The Department of Neurosurgery, Abbasi Shaheed Hospital, One Year Review StudyDokumen1 halamanResults of Various Modalities of Treatment For Acute Subdural Hematomas in The Department of Neurosurgery, Abbasi Shaheed Hospital, One Year Review Studyapi-19502000Belum ada peringkat
- In The Name of Allah The Beneficent The MercifulDokumen40 halamanIn The Name of Allah The Beneficent The Mercifulapi-19502000Belum ada peringkat
- Unintentional Durotomy During Spinal Surgeries Performed by The Department of Neurosurgery, Abbasi Shaheed Hospital Karachi A Two Years Review StudyDokumen1 halamanUnintentional Durotomy During Spinal Surgeries Performed by The Department of Neurosurgery, Abbasi Shaheed Hospital Karachi A Two Years Review Studyapi-19502000Belum ada peringkat
- Earthquake Relief Work in Baluchistan: 2 9 October, 2008Dokumen5 halamanEarthquake Relief Work in Baluchistan: 2 9 October, 2008api-19502000Belum ada peringkat
- ReadmeDokumen1 halamanReadmeapi-19502000Belum ada peringkat
- Islam The Misunderstood ReligionDokumen143 halamanIslam The Misunderstood ReligionEbtessamBelum ada peringkat
- Judgement Verdict Against Yusuf Kazzab Published in Book Form and Its Forward by Ismail Qureshi Adv Mentioning ZZ HamidDokumen10 halamanJudgement Verdict Against Yusuf Kazzab Published in Book Form and Its Forward by Ismail Qureshi Adv Mentioning ZZ Hamidjuggernaught313Belum ada peringkat
- Columns Obituaries - Psychiatrist pioneered mental healthcare in PakistanDokumen2 halamanColumns Obituaries - Psychiatrist pioneered mental healthcare in PakistanHaseeb DaudBelum ada peringkat
- Guidance on aptitude testingDokumen10 halamanGuidance on aptitude testingAntoBelum ada peringkat
- PHD Proposal - Ilan ValdesDokumen17 halamanPHD Proposal - Ilan ValdesIlan ValdesBelum ada peringkat
- Entire Research Proposal - NN ImDokumen3 halamanEntire Research Proposal - NN Imapi-546440127Belum ada peringkat
- Does Acupuncture Help Stroke Victims ImproveDokumen31 halamanDoes Acupuncture Help Stroke Victims ImprovetildateoBelum ada peringkat
- Coaching Observation AssignmentDokumen3 halamanCoaching Observation Assignmentapi-314123459Belum ada peringkat
- Spatial Neglect - Overview, Etiology, Mechanisms and Morbidities in Spatial NeglectDokumen9 halamanSpatial Neglect - Overview, Etiology, Mechanisms and Morbidities in Spatial NeglectRivulet1Belum ada peringkat
- Loud Music FunkDokumen2 halamanLoud Music FunkJosé de CarvalhoBelum ada peringkat
- Psicoterapia Sensoriomotora PDFDokumen974 halamanPsicoterapia Sensoriomotora PDFJosé Luis SH100% (4)
- Memory - Training Book With The Best TeacherDokumen43 halamanMemory - Training Book With The Best TeacherKassyano LopezBelum ada peringkat
- Types of ListeningDokumen2 halamanTypes of ListeningCrisalyn SicatBelum ada peringkat
- Chapter 2 Cognitive and Language DevelopmentDokumen12 halamanChapter 2 Cognitive and Language DevelopmentKristine ParafinaBelum ada peringkat
- Consumer Behaviour Model Question PaperDokumen2 halamanConsumer Behaviour Model Question PaperkarunasreemBelum ada peringkat
- Spector 2005Dokumen3 halamanSpector 2005arikusuma12Belum ada peringkat
- Edid6512 - Design Prospectus - Revised - Nyeisha George-MinottDokumen13 halamanEdid6512 - Design Prospectus - Revised - Nyeisha George-Minottapi-298012003100% (1)
- Stop CrammingDokumen6 halamanStop CrammingCharmaine AlipayoBelum ada peringkat
- Autoimmune Encephalitis Syndromes With Antibodies - UpToDateDokumen1 halamanAutoimmune Encephalitis Syndromes With Antibodies - UpToDateSamBelum ada peringkat
- Whitney Mclaughlin 2019 Ncca PresentationDokumen21 halamanWhitney Mclaughlin 2019 Ncca Presentationapi-298976119Belum ada peringkat
- Ursula E. Oberst, Alan E. Stewart - Adlerian Psych PDFDokumen235 halamanUrsula E. Oberst, Alan E. Stewart - Adlerian Psych PDFRadu PrusanBelum ada peringkat
- Conceptual FrameworkDokumen10 halamanConceptual FrameworkMeynard AndresBelum ada peringkat
- Personal DevelopmewntDokumen14 halamanPersonal DevelopmewntKeneth Rose FagtananBelum ada peringkat
- Human BehaviorDokumen133 halamanHuman BehaviorLeslie Joy Edrosolo ColomaBelum ada peringkat
- CommunicationDokumen20 halamanCommunicationPrajakta GokhaleBelum ada peringkat
- Psychological Processes in Language Learning and Teaching: Methods and Approaches of PsycholinguisticsDokumen7 halamanPsychological Processes in Language Learning and Teaching: Methods and Approaches of PsycholinguisticsMohamed IZZ El-DeenBelum ada peringkat
- Dissociative Identity DisorderDokumen16 halamanDissociative Identity Disorderapi-453434906Belum ada peringkat
- Depression in Men OPED - Dr. MugambiDokumen3 halamanDepression in Men OPED - Dr. MugambiCosmas MugambiBelum ada peringkat
- IB Psych Biological Level - Revision NotesDokumen2 halamanIB Psych Biological Level - Revision NotesNoor MohsinBelum ada peringkat