Anda mungkin juga menyukai
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Anatomy Quizbook PDFDokumen92 halamanAnatomy Quizbook PDFLipid Berger67% (3)
- Pulmonary Embolism: Signs and SymptomsDokumen4 halamanPulmonary Embolism: Signs and SymptomsSeth KnightsBelum ada peringkat
- Pulmonary Bleb: On This PageDokumen6 halamanPulmonary Bleb: On This PageYaumul RobbiBelum ada peringkat
- Unitor Alkalinity ControlDokumen14 halamanUnitor Alkalinity Controlamin32Belum ada peringkat
- Parts & Function of Respiratory SystemDokumen4 halamanParts & Function of Respiratory SystemLucille Ballares83% (6)
- Chapter 28: Obstructive Pulmonary Diseases Harding: Lewis's Medical-Surgical Nursing, 11th EditionDokumen15 halamanChapter 28: Obstructive Pulmonary Diseases Harding: Lewis's Medical-Surgical Nursing, 11th EditionKrishna RamaBelum ada peringkat
- Mbbs PhysioDokumen27 halamanMbbs PhysioWwwanand111Belum ada peringkat
- Anatomy MCQ Abdomen and ThoraxDokumen168 halamanAnatomy MCQ Abdomen and ThoraxRobert Edwards77% (22)
- Tissues Organs and Systems-9 7 15Dokumen2 halamanTissues Organs and Systems-9 7 15api-294498352100% (1)
- 50 Nursing Mnemonics and Acronyms You Need To Know NowDokumen29 halaman50 Nursing Mnemonics and Acronyms You Need To Know Nowtandz100% (19)
- Chapter 6 Life Processes For Class 10 BiologyDokumen15 halamanChapter 6 Life Processes For Class 10 BiologyKhushi RochwaniBelum ada peringkat
- Clinical Examination of The Thorax, Abdomen and PelvisDokumen42 halamanClinical Examination of The Thorax, Abdomen and PelvisTunnelssBelum ada peringkat
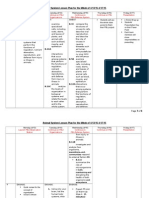
- Animal System Lesson PlanDokumen6 halamanAnimal System Lesson Planapi-266567690Belum ada peringkat
- Dissertation Report SpirometerDokumen40 halamanDissertation Report SpirometerAbhishek RajanBelum ada peringkat
- Edge Detection From CT Images of Lung: Prof. Samir Kumar BandyopadhyayDokumen4 halamanEdge Detection From CT Images of Lung: Prof. Samir Kumar BandyopadhyayIjesat JournalBelum ada peringkat
- Dr. Dicky Soehardiman - Seawater Vs FreshwaterDokumen1 halamanDr. Dicky Soehardiman - Seawater Vs FreshwaterIGD RSMYBelum ada peringkat
- Blossom 19 Petal 2 2Dokumen10 halamanBlossom 19 Petal 2 2Ram SinghBelum ada peringkat
- Biology 20 Unit Plan Circulation and Gas ExchangeDokumen3 halamanBiology 20 Unit Plan Circulation and Gas Exchangeapi-332074447Belum ada peringkat
- Major Body OrgansDokumen28 halamanMajor Body Organsesang quettBelum ada peringkat
- Step Notes: RRC SampleDokumen9 halamanStep Notes: RRC SampleRafia 0205Belum ada peringkat
- MTHISTO100 Lesson 2 Respiratory SystemDokumen7 halamanMTHISTO100 Lesson 2 Respiratory SystemJaeri HuangBelum ada peringkat
- Sustaining The Earth 10th Edition Miller Test BankDokumen25 halamanSustaining The Earth 10th Edition Miller Test BankTylerArcherrgcax100% (33)
- Activity SheetsDokumen6 halamanActivity SheetsDarrelRagotBelum ada peringkat
- Textbook of Respiratory Disease in Dogs and Cats Parasites of The LungDokumen12 halamanTextbook of Respiratory Disease in Dogs and Cats Parasites of The LungDiego CushicóndorBelum ada peringkat
- Respiratory FailureDokumen39 halamanRespiratory FailureMuntasir BashirBelum ada peringkat
- Class ReptiliaDokumen8 halamanClass ReptiliaKuromiksBelum ada peringkat
- Guide To Less Toxic ProductsDokumen103 halamanGuide To Less Toxic ProductsAB100% (1)
- Narrative PathophysiologyDokumen18 halamanNarrative PathophysiologyNica Georgelle Maniego SamonteBelum ada peringkat
- Science Form 1 Chapter 2Dokumen29 halamanScience Form 1 Chapter 2qq23588% (68)
- Grade 9Dokumen3 halamanGrade 9Salve Gregorio AguirreBelum ada peringkat