Anda mungkin juga menyukai
- Step-By-Step Instructions On The: Straumann TibrushDokumen4 halamanStep-By-Step Instructions On The: Straumann Tibrushadambear213Belum ada peringkat
- JadaDokumen14 halamanJadaadambear213Belum ada peringkat
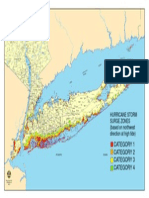
- Nys Storm Surge ZonesDokumen1 halamanNys Storm Surge Zonesadambear213Belum ada peringkat
- Sterile Healing Solutions FOFDokumen2 halamanSterile Healing Solutions FOFadambear213Belum ada peringkat
- Greenstein Et Tarnow 2006ddDokumen11 halamanGreenstein Et Tarnow 2006ddAnup Lal RajbahakBelum ada peringkat
- Keratinized Mucosa Around Dental ImplantsDokumen2 halamanKeratinized Mucosa Around Dental Implantsadambear213Belum ada peringkat
- Periodontal Dictates For Esthetic Ceramometal Crowns: R - Sheldon Stein, DMDDokumen11 halamanPeriodontal Dictates For Esthetic Ceramometal Crowns: R - Sheldon Stein, DMDadambear213Belum ada peringkat
- CDC - Half of American Adults Have Periodontal Disease - PerioDokumen3 halamanCDC - Half of American Adults Have Periodontal Disease - Perioadambear213Belum ada peringkat
- Jop 1974 45 3 151Dokumen4 halamanJop 1974 45 3 151adambear213Belum ada peringkat
- Malpractice and Perio DiseaseDokumen4 halamanMalpractice and Perio Diseaseadambear213Belum ada peringkat
- Dental Office Marketing PlanDokumen20 halamanDental Office Marketing PlanPalo Alto Software100% (10)
- 27Dokumen7 halaman27adambear213Belum ada peringkat
- ArticleDokumen7 halamanArticleadambear213Belum ada peringkat
- REVISED ASSIGNMENTS Biology and Pathology of The PeriodontiumDokumen2 halamanREVISED ASSIGNMENTS Biology and Pathology of The Periodontiumadambear213Belum ada peringkat
- 3-Evaluation of Human Recession Defects Treated With Coronally Advanced Flaps and Either Enamel Matrix Derivatives or Connective Tissue - Comparison of Clinical Parameters at 10Dokumen10 halaman3-Evaluation of Human Recession Defects Treated With Coronally Advanced Flaps and Either Enamel Matrix Derivatives or Connective Tissue - Comparison of Clinical Parameters at 10adambear213Belum ada peringkat
- WhatsNew EDokumen37 halamanWhatsNew Eadambear213Belum ada peringkat
- Ideas Academy Reports: and InnovationsDokumen9 halamanIdeas Academy Reports: and Innovationsadambear213Belum ada peringkat
- Average Tooth MeasurmentsDokumen1 halamanAverage Tooth Measurmentsadambear213Belum ada peringkat
- IBR Application CDokumen12 halamanIBR Application CChris HudginsBelum ada peringkat
- 16Dokumen9 halaman16adambear213Belum ada peringkat
- J 1600-0757 1997 tb00094 XDokumen21 halamanJ 1600-0757 1997 tb00094 Xadambear213Belum ada peringkat
- WhatsNew E OldDokumen25 halamanWhatsNew E Oldadambear213Belum ada peringkat
- Suture Surg Gut Chrom Bge FS2 4Dokumen1 halamanSuture Surg Gut Chrom Bge FS2 4adambear213Belum ada peringkat
- Map ArenaDokumen1 halamanMap Arenaadambear213Belum ada peringkat
- Sterile Healing Solutions FOFDokumen2 halamanSterile Healing Solutions FOFadambear213Belum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Chest Drain Management GuideDokumen11 halamanChest Drain Management GuideRaina Ginella DsouzaBelum ada peringkat
- Extra-Oral Radiology DR Vineetha 2003 FormatDokumen7 halamanExtra-Oral Radiology DR Vineetha 2003 FormatEshan VermaBelum ada peringkat
- Clausen 001Dokumen9 halamanClausen 001api-301171718Belum ada peringkat
- Evaluation ToolDokumen3 halamanEvaluation Toolbulikako100% (1)
- Gastroscope Gve-2100Dokumen22 halamanGastroscope Gve-2100Victor BlancoBelum ada peringkat
- Diagnostic Laparoscopy: Reason For VisitDokumen4 halamanDiagnostic Laparoscopy: Reason For Visitdrnareshkumar3281Belum ada peringkat
- Back Pain QuestionnaireDokumen2 halamanBack Pain QuestionnaireiikemBelum ada peringkat
- FamcourtDokumen3 halamanFamcourtManders BuchmanBelum ada peringkat
- Perio Notes CombinedDokumen71 halamanPerio Notes CombinedHayley WelshBelum ada peringkat
- Relaxation in Hypertension PDFDokumen8 halamanRelaxation in Hypertension PDFSzerenaBelum ada peringkat
- Stress Related DiseasesDokumen32 halamanStress Related DiseasesIacob Alin100% (1)
- Final Exam (Leadeship and Management)Dokumen10 halamanFinal Exam (Leadeship and Management)Jessica M. AsiseoBelum ada peringkat
- Vertebrobasilar Ischemic Stroke Diagnosis and TreatmentDokumen35 halamanVertebrobasilar Ischemic Stroke Diagnosis and TreatmentBen Asiel PadangBelum ada peringkat
- Led Light Therapy GuideDokumen23 halamanLed Light Therapy GuidePeter Freimann100% (4)
- Managing The MismatchDokumen36 halamanManaging The MismatchhumansamirBelum ada peringkat
- Yalom Momma and The Meaning of LifeDokumen15 halamanYalom Momma and The Meaning of LifeKatya Black0% (1)
- Early Postoperative Treatment of Surgical Scars Using A Fractional Carbon Dioxide LaserDokumen7 halamanEarly Postoperative Treatment of Surgical Scars Using A Fractional Carbon Dioxide LaserdoctorbanBelum ada peringkat
- Interviewing When FamilyDokumen4 halamanInterviewing When FamilygabrielaBelum ada peringkat
- Epigastric Pain and Management of FeverDokumen41 halamanEpigastric Pain and Management of FeverAkhr RiBelum ada peringkat
- Brain Anatomy and Methods to Study CognitionDokumen30 halamanBrain Anatomy and Methods to Study CognitionJuliana FeronBelum ada peringkat
- 40-Article Text-119-1-10-20151207Dokumen13 halaman40-Article Text-119-1-10-20151207Guna SoundariBelum ada peringkat
- 2002 Solution-Focused Brief TherapyDokumen9 halaman2002 Solution-Focused Brief Therapymgnpni100% (1)
- Case Control StudiesDokumen30 halamanCase Control StudiesSana AfreenBelum ada peringkat
- My Thesis Protocol-4Dokumen15 halamanMy Thesis Protocol-4Rio RockyBelum ada peringkat
- Asepsis and Infection Control Nursing SchoolDokumen20 halamanAsepsis and Infection Control Nursing Schoolleonardo orozco100% (1)
- Early Warning ScoreDokumen8 halamanEarly Warning ScoremalleshmadeshBelum ada peringkat
- Grammar Vocabulary 2star Unit3 PDFDokumen2 halamanGrammar Vocabulary 2star Unit3 PDFLorenaAbreuBelum ada peringkat
- DM AAFP ManagementDokumen8 halamanDM AAFP ManagementphilsguBelum ada peringkat
- Management of StrokeDokumen24 halamanManagement of StrokeEngel TuranganBelum ada peringkat
- Xodo Document - Periprocedural - Anticoagulation - GuidelineDokumen16 halamanXodo Document - Periprocedural - Anticoagulation - Guidelinebrigde_xBelum ada peringkat