Anda mungkin juga menyukai
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Present Tense Exercises. Polish A1Dokumen6 halamanPresent Tense Exercises. Polish A1Pilar Moreno DíezBelum ada peringkat
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Family Medicine Residents Orthopedic Rotation HandoutDokumen18 halamanFamily Medicine Residents Orthopedic Rotation HandoutRuth PoeryBelum ada peringkat
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- APFC Accountancy Basic Study Material For APFCEPFO ExamDokumen3 halamanAPFC Accountancy Basic Study Material For APFCEPFO ExamIliasBelum ada peringkat
- Death and DickinsonDokumen12 halamanDeath and DickinsonHarshita Sohal100% (1)
- Keppel's lease rights and option to purchase land upheldDokumen6 halamanKeppel's lease rights and option to purchase land upheldkdcandariBelum ada peringkat
- Basic Concepts of Fluid and Electrolyte TherapyDokumen136 halamanBasic Concepts of Fluid and Electrolyte Therapynoorgianilestari100% (2)
- Portfolio Management Services-Hrithik JainDokumen73 halamanPortfolio Management Services-Hrithik Jain8784100% (1)
- Trends, Networks, and Critical Thinking in The 21st CenturyDokumen22 halamanTrends, Networks, and Critical Thinking in The 21st CenturyGabrelle Ogayon100% (1)
- Business Plan Presentation ON Air Conditioner: Presented By-V.Sowmith REG NO-2121BM010112Dokumen16 halamanBusiness Plan Presentation ON Air Conditioner: Presented By-V.Sowmith REG NO-2121BM010112Kavya Madanu100% (1)
- Lebel Contoh PrintDokumen1 halamanLebel Contoh PrintnoorgianilestariBelum ada peringkat
- Kahlil Gibran Part ViiDokumen1 halamanKahlil Gibran Part ViinoorgianilestariBelum ada peringkat
- Daftar Pustaka Hipertensi, Diabetes dan AsmaDokumen2 halamanDaftar Pustaka Hipertensi, Diabetes dan AsmanoorgianilestariBelum ada peringkat
- Medical Disciplinary-Tugas Prof EkaDokumen3 halamanMedical Disciplinary-Tugas Prof EkanoorgianilestariBelum ada peringkat
- Body Dysmorphic TraynorDokumen12 halamanBody Dysmorphic TraynornoorgianilestariBelum ada peringkat
- ACHMDokumen1 halamanACHMnoorgianilestariBelum ada peringkat
- Supraventricular TachycardiaDokumen37 halamanSupraventricular TachycardianoorgianilestariBelum ada peringkat
- Pa To GenesisDokumen1 halamanPa To GenesisnoorgianilestariBelum ada peringkat
- Proteomic ReportDokumen25 halamanProteomic ReportnoorgianilestariBelum ada peringkat
- Van Den Berghe G, Wouters P, Weekers F, Et Al. Intensive Insulin Therapy in Critically Ill Patients. N Engl J Med 345: 1359-1367, 2001Dokumen1 halamanVan Den Berghe G, Wouters P, Weekers F, Et Al. Intensive Insulin Therapy in Critically Ill Patients. N Engl J Med 345: 1359-1367, 2001noorgianilestariBelum ada peringkat
- Van Den Berghe G, Wouters P, Weekers F, Et Al. Intensive Insulin Therapy in Critically Ill Patients. N Engl J Med 345: 1359-1367, 2001Dokumen1 halamanVan Den Berghe G, Wouters P, Weekers F, Et Al. Intensive Insulin Therapy in Critically Ill Patients. N Engl J Med 345: 1359-1367, 2001noorgianilestariBelum ada peringkat
- Hasil UrinalysisDokumen1 halamanHasil UrinalysisnoorgianilestariBelum ada peringkat
- Jadwal Koas IPDDokumen11 halamanJadwal Koas IPDnoorgianilestariBelum ada peringkat
- LO Week 5Dokumen6 halamanLO Week 5noorgianilestariBelum ada peringkat
- Visum et repertum report 1 October 2014Dokumen4 halamanVisum et repertum report 1 October 2014noorgianilestariBelum ada peringkat
- WEEK Orthopedics DR JohnDokumen16 halamanWEEK Orthopedics DR JohnnoorgianilestariBelum ada peringkat
- Blood TransfusionDokumen30 halamanBlood TransfusionnoorgianilestariBelum ada peringkat
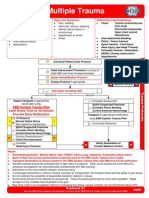
- Multiple Trauma: EMS System Trauma Plan Limit Scene Time To 10 Minutes Provide Early NotificationDokumen1 halamanMultiple Trauma: EMS System Trauma Plan Limit Scene Time To 10 Minutes Provide Early NotificationKelly JacksonBelum ada peringkat
- Diagnosis MeningitisDokumen25 halamanDiagnosis MeningitisnoorgianilestariBelum ada peringkat
- CiminoDokumen2 halamanCiminonoorgianilestariBelum ada peringkat
- Diagnosis MeningitisDokumen25 halamanDiagnosis MeningitisnoorgianilestariBelum ada peringkat
- Otitis Media AkutDokumen9 halamanOtitis Media AkutnoorgianilestariBelum ada peringkat
- Revision and Second Term TestDokumen15 halamanRevision and Second Term TestThu HươngBelum ada peringkat
- Salzer Panel Accessories Price List - 01st January 2019Dokumen40 halamanSalzer Panel Accessories Price List - 01st January 2019Chandra SekaranBelum ada peringkat
- Mobile Services Tax Invoice for Dr Reddys LaboratoriesDokumen3 halamanMobile Services Tax Invoice for Dr Reddys LaboratoriesK Sree RamBelum ada peringkat
- IT WorkShop Lab ManualDokumen74 halamanIT WorkShop Lab ManualcomputerstudentBelum ada peringkat
- Keyboard notes to Fur Elise melodyDokumen2 halamanKeyboard notes to Fur Elise melodyReji SarsalejoBelum ada peringkat
- The Man of Sorrows Wednesday of Holy Week Divine IntimacyDokumen5 halamanThe Man of Sorrows Wednesday of Holy Week Divine IntimacyTerri ThomasBelum ada peringkat
- Chapter 3 - The Role of Multimedia in EducationDokumen37 halamanChapter 3 - The Role of Multimedia in EducationGellie Ann Silvestre RapinBelum ada peringkat
- Module 1 in Contemporary Arts First MonthDokumen12 halamanModule 1 in Contemporary Arts First MonthMiles Bugtong CagalpinBelum ada peringkat
- Bakhtar University: Graduate School of Business AdministrationDokumen3 halamanBakhtar University: Graduate School of Business AdministrationIhsanulhaqnooriBelum ada peringkat
- Fernando Medical Enterprises, Inc. v. Wesleyan University Phils., Inc.Dokumen10 halamanFernando Medical Enterprises, Inc. v. Wesleyan University Phils., Inc.Clement del RosarioBelum ada peringkat
- AefiDokumen38 halamanAefizedregga2Belum ada peringkat
- 4 FIN555 Chap 4 Prings Typical Parameters For Intermediate Trend (Recovered)Dokumen16 halaman4 FIN555 Chap 4 Prings Typical Parameters For Intermediate Trend (Recovered)Najwa SulaimanBelum ada peringkat
- Land Securities Group (A)Dokumen13 halamanLand Securities Group (A)Piyush SamalBelum ada peringkat
- EDUC 5240 - Creating Positive Classroom EnvironmentsDokumen5 halamanEDUC 5240 - Creating Positive Classroom EnvironmentsMay Phyo ThuBelum ada peringkat
- Dukic WarehouselayoutsDokumen14 halamanDukic Warehouselayoutsrohitkamath7Belum ada peringkat
- SalutogenicshandbookDokumen16 halamanSalutogenicshandbookAna EclipseBelum ada peringkat
- Bracketing MethodsDokumen13 halamanBracketing Methodsasd dsa100% (1)
- Fitting A Logistic Curve To DataDokumen12 halamanFitting A Logistic Curve To DataXiaoyan ZouBelum ada peringkat
- Pashmina vs Cashmere: Which Luxury Fiber Is SofterDokumen15 halamanPashmina vs Cashmere: Which Luxury Fiber Is SofterSJVN CIVIL DESIGN100% (1)
- Calvo, G (1988) - Servicing The Public Debt - The Role of ExpectationsDokumen16 halamanCalvo, G (1988) - Servicing The Public Debt - The Role of ExpectationsDaniela SanabriaBelum ada peringkat
- Zeal Study 10th English Synonym Unit 1 - 7Dokumen24 halamanZeal Study 10th English Synonym Unit 1 - 7viaanenterprises2008Belum ada peringkat
- Community ResourcesDokumen30 halamanCommunity Resourcesapi-242881060Belum ada peringkat
- Entrepreneurship - Quarter 2 - Week 1-3 - 4 M's of Production and - Business ModelDokumen6 halamanEntrepreneurship - Quarter 2 - Week 1-3 - 4 M's of Production and - Business ModelJude Del RosarioBelum ada peringkat