Anda mungkin juga menyukai
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5782)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Master Your FinancesDokumen15 halamanMaster Your FinancesBrendan GirdwoodBelum ada peringkat
- 3 QDokumen2 halaman3 QJerahmeel CuevasBelum ada peringkat
- v6c. Story of CarbonDokumen12 halamanv6c. Story of CarbonJahangir AliBelum ada peringkat
- Here Late?", She Asked Me.: TrangDokumen3 halamanHere Late?", She Asked Me.: TrangNguyễn Đình TrọngBelum ada peringkat
- SK Council Authorizes New Bank AccountDokumen3 halamanSK Council Authorizes New Bank Accountt3emo shikihiraBelum ada peringkat
- Israel Bible MapDokumen1 halamanIsrael Bible MapMoses_JakkalaBelum ada peringkat
- ZZXCDokumen2 halamanZZXCKrisleen AbrenicaBelum ada peringkat
- NDA Template Non Disclosure Non Circumvent No Company NameDokumen9 halamanNDA Template Non Disclosure Non Circumvent No Company NamepvorsterBelum ada peringkat
- SEIPIDokumen20 halamanSEIPIdexterbautistadecember161985Belum ada peringkat
- Supplier of PesticidesDokumen2 halamanSupplier of PesticidestusharBelum ada peringkat
- BAFINAR - Midterm Draft (R) PDFDokumen11 halamanBAFINAR - Midterm Draft (R) PDFHazel Iris Caguingin100% (1)
- Teacher swap agreement for family reasonsDokumen4 halamanTeacher swap agreement for family reasonsKimber LeeBelum ada peringkat
- dlp4 Math7q3Dokumen3 halamandlp4 Math7q3Therence UbasBelum ada peringkat
- Oilwell Fishing Operations Tools and TechniquesDokumen126 halamanOilwell Fishing Operations Tools and Techniqueskevin100% (2)
- Relay Models Per Types Mdp38 EnuDokumen618 halamanRelay Models Per Types Mdp38 Enuazer NadingaBelum ada peringkat
- Sky Education: Organisation of Commerce and ManagementDokumen12 halamanSky Education: Organisation of Commerce and ManagementKiyaara RathoreBelum ada peringkat
- Total Product Marketing Procedures: A Case Study On "BSRM Xtreme 500W"Dokumen75 halamanTotal Product Marketing Procedures: A Case Study On "BSRM Xtreme 500W"Yasir Alam100% (1)
- Financial Management Module - 3Dokumen2 halamanFinancial Management Module - 3Roel AsduloBelum ada peringkat
- Training of Local Government Personnel PHDokumen5 halamanTraining of Local Government Personnel PHThea ConsBelum ada peringkat
- Week 5 WHLP Nov. 2 6 2020 DISSDokumen5 halamanWeek 5 WHLP Nov. 2 6 2020 DISSDaniel BandibasBelum ada peringkat
- Soil Mechanics: Principle of Effective Stress, Capillarity and Permeability On SoilDokumen54 halamanSoil Mechanics: Principle of Effective Stress, Capillarity and Permeability On SoilAwadhiBelum ada peringkat
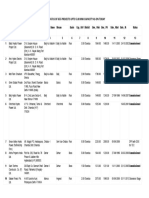
- List/Status of 655 Projects Upto 5.00 MW Capacity As On TodayDokumen45 halamanList/Status of 655 Projects Upto 5.00 MW Capacity As On Todayganvaqqqzz21Belum ada peringkat
- History of Downtown San Diego - TimelineDokumen3 halamanHistory of Downtown San Diego - Timelineapi-671103457Belum ada peringkat
- ICU Lines TubesDokumen7 halamanICU Lines TubesCindy MurphyBelum ada peringkat
- ICE Learned Event DubaiDokumen32 halamanICE Learned Event DubaiengkjBelum ada peringkat
- 9 Specific Relief Act, 1877Dokumen20 halaman9 Specific Relief Act, 1877mostafa faisalBelum ada peringkat
- Hac 1001 NotesDokumen56 halamanHac 1001 NotesMarlin MerikanBelum ada peringkat
- Business Data Communications and Networking 13Th Edition Fitzgerald Test Bank Full Chapter PDFDokumen40 halamanBusiness Data Communications and Networking 13Th Edition Fitzgerald Test Bank Full Chapter PDFthrongweightypfr100% (12)
- HLT42707 Certificate IV in Aromatherapy: Packaging RulesDokumen2 halamanHLT42707 Certificate IV in Aromatherapy: Packaging RulesNilamdeen Mohamed ZamilBelum ada peringkat
- Genocide/Politicides, 1954-1998 - State Failure Problem SetDokumen9 halamanGenocide/Politicides, 1954-1998 - State Failure Problem SetSean KimBelum ada peringkat