Anda mungkin juga menyukai
- PEAK Restoration of The Endodontically Treated Tooth PDFDokumen20 halamanPEAK Restoration of The Endodontically Treated Tooth PDFana9025100% (1)
- (Stem Cell Biology and Regenerative Medicine) Marco Tatullo (Eds.) - MSCs and Innovative Biomaterials in Dentistry-Humana Press (2017)Dokumen199 halaman(Stem Cell Biology and Regenerative Medicine) Marco Tatullo (Eds.) - MSCs and Innovative Biomaterials in Dentistry-Humana Press (2017)chenBelum ada peringkat
- Treatment Planning Single Maxillary Anterior Implants for DentistsDari EverandTreatment Planning Single Maxillary Anterior Implants for DentistsBelum ada peringkat
- PEAK Restoration of The Endodontically Treated ToothDokumen20 halamanPEAK Restoration of The Endodontically Treated Toothlishenwong100% (1)
- Completedenture Theory and PracticeDokumen1.233 halamanCompletedenture Theory and PracticeMostafa Fayad100% (7)
- AHA ALS Instructor Manual Ucm - 499297Dokumen58 halamanAHA ALS Instructor Manual Ucm - 499297Khalid G. AzouniBelum ada peringkat
- The "Index Technique" in Worn Dentition: A New and Conservative ApproachDokumen32 halamanThe "Index Technique" in Worn Dentition: A New and Conservative ApproachHektor Hak100% (1)
- Gingival Recession and Various Root Coverage ProceduresDokumen6 halamanGingival Recession and Various Root Coverage ProceduresKhalid G. AzouniBelum ada peringkat
- Gingival Recession and Various Root Coverage ProceduresDokumen6 halamanGingival Recession and Various Root Coverage ProceduresKhalid G. AzouniBelum ada peringkat
- Prostho-Perio-Restorative Interrelationship ADokumen6 halamanProstho-Perio-Restorative Interrelationship AAlipio GarcíaBelum ada peringkat
- Dental Enamel: Dr. Prabhat Saxena Dept of Endodontics S.G.T. Dental College, GurgaonDokumen114 halamanDental Enamel: Dr. Prabhat Saxena Dept of Endodontics S.G.T. Dental College, GurgaonPrabhat Saxena100% (1)
- Justification For Orthodontic TreatmentDokumen16 halamanJustification For Orthodontic TreatmentAries ZodiackBelum ada peringkat
- ADC Exam - MCQDokumen10 halamanADC Exam - MCQHatem Abouelnasr100% (10)
- European Resuscitation Council Guidelines 2021Dokumen468 halamanEuropean Resuscitation Council Guidelines 2021Khalid G. AzouniBelum ada peringkat
- Dentin Hypersensitivity SeminarDokumen91 halamanDentin Hypersensitivity SeminarBharat Singh ChauhanBelum ada peringkat
- Operative Dentistry A Threat To Pulp PDFDokumen5 halamanOperative Dentistry A Threat To Pulp PDFAnonymous 5IYvZnE5Belum ada peringkat
- The "Index Technique" in Worn Dentition - A New and Conservative ApproachDokumen32 halamanThe "Index Technique" in Worn Dentition - A New and Conservative ApproachFilipe Queiroz100% (2)
- The Aetiology of Gingival RecessionDokumen4 halamanThe Aetiology of Gingival RecessionshahidibrarBelum ada peringkat
- Vital PulpectomyDokumen39 halamanVital PulpectomySoo YoongBelum ada peringkat
- Pulpal & Dental PainDokumen28 halamanPulpal & Dental PainAli Al-Qudsi100% (1)
- Vital Pulp Ricucci PDFDokumen12 halamanVital Pulp Ricucci PDFBeto O Rivero100% (1)
- How Biomechanics Can Affect The Endodontic Treated Teeth and Their Restorative ProceduresDokumen15 halamanHow Biomechanics Can Affect The Endodontic Treated Teeth and Their Restorative ProceduresEdward AbadiaBelum ada peringkat
- EJED1 Dietschi PDFDokumen14 halamanEJED1 Dietschi PDFAdriana Coronado100% (1)
- Vailatti Palatal VeneersDokumen11 halamanVailatti Palatal VeneersDurbal Antonio MontecinosBelum ada peringkat
- Post Operative Sensitivity On Direct ResDokumen12 halamanPost Operative Sensitivity On Direct ResComarzzoBelum ada peringkat
- Non-Carious Cervical Lesion: Case Report: Roberta C. G. Terra, Isis A. V. P. Poiate and Edgard Poiate JRDokumen4 halamanNon-Carious Cervical Lesion: Case Report: Roberta C. G. Terra, Isis A. V. P. Poiate and Edgard Poiate JRAgum Nila Sari IIBelum ada peringkat
- New Direct Resilient Relining Material of Denture Base: International Medical Journal (1994) April 2018Dokumen4 halamanNew Direct Resilient Relining Material of Denture Base: International Medical Journal (1994) April 2018lulukzBelum ada peringkat
- Management of Periodontally Involved Anterior Teeth by Glass Fiber-Reinforced Composite Splinting: A Clinical Report With 5-Year RecallDokumen6 halamanManagement of Periodontally Involved Anterior Teeth by Glass Fiber-Reinforced Composite Splinting: A Clinical Report With 5-Year RecallmarethadwiBelum ada peringkat
- Preserving The Vital Pulp in Operative Dentistry: 2. Guidelines For Successful Restoration of Unexposed Dentinal LesionsDokumen7 halamanPreserving The Vital Pulp in Operative Dentistry: 2. Guidelines For Successful Restoration of Unexposed Dentinal LesionsRadhikaManamBelum ada peringkat
- OunsiDokumen7 halamanOunsiDanis Diba Sabatillah YaminBelum ada peringkat
- Avulsion: DEFINITION: - Tooth Avulsion (Exarticulation) Implies Total Displacement of The ToothDokumen39 halamanAvulsion: DEFINITION: - Tooth Avulsion (Exarticulation) Implies Total Displacement of The Toothshailesh_shenoyBelum ada peringkat
- 32 V PDFDokumen7 halaman32 V PDFNabil AlkaffBelum ada peringkat
- Crown Lengthening Vs Forced EruptionDokumen4 halamanCrown Lengthening Vs Forced EruptionbarbieBelum ada peringkat
- Soft Tissues DisplacementDokumen39 halamanSoft Tissues DisplacementKhaled ElshabrawyBelum ada peringkat
- Extreme Root Resorption Associated With Induced Tooth Movement - A Protocol For Clinical ManagementDokumen8 halamanExtreme Root Resorption Associated With Induced Tooth Movement - A Protocol For Clinical Managementcarmen espinozaBelum ada peringkat
- Retrieve 39Dokumen23 halamanRetrieve 39Freddy BenalcázarBelum ada peringkat
- Murray2002 PDFDokumen10 halamanMurray2002 PDFTulasi CpBelum ada peringkat
- 1 s2.0 S0109564113001814 MainDokumen7 halaman1 s2.0 S0109564113001814 MainNarcisa TabarceaBelum ada peringkat
- DentalImplants AReviewDokumen26 halamanDentalImplants AReviewDoménica ManriqueBelum ada peringkat
- About I 2001Dokumen9 halamanAbout I 2001Ricardo Rodrigues AmaralBelum ada peringkat
- Adhesive Restorations Centric RelationDokumen14 halamanAdhesive Restorations Centric RelationIlse100% (1)
- DentalImplants AReview1 PDFDokumen21 halamanDentalImplants AReview1 PDFDhanu DhanushreeBelum ada peringkat
- Article1404395371 - Shibu and RajanDokumen3 halamanArticle1404395371 - Shibu and RajanRuchi ShahBelum ada peringkat
- Guia Anterior - Gonzalez Hernandez-61-2Dokumen12 halamanGuia Anterior - Gonzalez Hernandez-61-2Fred TorresBelum ada peringkat
- Prosthodontics PDFDokumen27 halamanProsthodontics PDFزهراء فاضل اجبير فعيل100% (1)
- Management of Tooth Resorption PDFDokumen17 halamanManagement of Tooth Resorption PDFMohammed Omosh100% (1)
- Adhesive Dental Materials-A Review: John W. NicholsonDokumen8 halamanAdhesive Dental Materials-A Review: John W. NicholsonKaustav MandalBelum ada peringkat
- Periodontal Restorative Inter-Relationship: A ReviewDokumen9 halamanPeriodontal Restorative Inter-Relationship: A ReviewKrupali JainBelum ada peringkat
- Dental Implant MaintenanceDokumen7 halamanDental Implant MaintenanceLalaBelum ada peringkat
- Direct Restoration of Endodontically Treated Teeth A Brief Sumary of Materials and TechnoquesDokumen8 halamanDirect Restoration of Endodontically Treated Teeth A Brief Sumary of Materials and Technoquesmaroun ghalebBelum ada peringkat
- Recall Examinations Are Especially Important For Patients With Extensive Restorations and ShouldDokumen5 halamanRecall Examinations Are Especially Important For Patients With Extensive Restorations and Shouldverena milaBelum ada peringkat
- Pin-Retained Restoration With Resin Bonded Composite of A Badly Broken ToothDokumen3 halamanPin-Retained Restoration With Resin Bonded Composite of A Badly Broken ToothIOSRjournalBelum ada peringkat
- Features of The Clinical Course of Pulpitis in Temporary Teeth in ChildrenDokumen5 halamanFeatures of The Clinical Course of Pulpitis in Temporary Teeth in ChildrenCentral Asian StudiesBelum ada peringkat
- Bonding and Debonding From Metal To Ceramic: Research and Its Clinical ApplicationDokumen13 halamanBonding and Debonding From Metal To Ceramic: Research and Its Clinical Applicationgriffone1Belum ada peringkat
- 322 1403 1 PB PDFDokumen2 halaman322 1403 1 PB PDFAdityaBelum ada peringkat
- Bleaching3 Konser2Dokumen3 halamanBleaching3 Konser2akmalsatibiBelum ada peringkat
- Pulp IrritantsDokumen8 halamanPulp IrritantsKarma YogaBelum ada peringkat
- 29.D17 384 Muhammad Harun Achmad4 PDFDokumen7 halaman29.D17 384 Muhammad Harun Achmad4 PDFDeviBelum ada peringkat
- Occurrence and Causing Stimuli of Postoperative Sensitivity in Composite Restorations PDFDokumen8 halamanOccurrence and Causing Stimuli of Postoperative Sensitivity in Composite Restorations PDFDavid ColonBelum ada peringkat
- Ejpd 2017 1 5Dokumen5 halamanEjpd 2017 1 5Mariatun Zahro NasutionBelum ada peringkat
- Banerjee - 2018 - Selective Removal of Carious DentinDokumen16 halamanBanerjee - 2018 - Selective Removal of Carious DentinAli Al-QaysiBelum ada peringkat
- Vital Pulp Therapy Using Calcium-Enriched Mixture An Evidence-Based ReviewDokumen8 halamanVital Pulp Therapy Using Calcium-Enriched Mixture An Evidence-Based ReviewRobin FernandezBelum ada peringkat
- PCD N FRCDokumen11 halamanPCD N FRCDebora GultomBelum ada peringkat
- Art I Go OverlayDokumen10 halamanArt I Go OverlayPaulette Sarmiento RosalesBelum ada peringkat
- [International Endodontic Journal 2017-Jul 26 Vol. 51] Nazzal, H_ Kenny, K_ Altimimi, A_ Kang, J_ Duggal, M S - A Prospective Clinical Study of Regenerative Endodontic Treatment of Traumatised Immature Teeth With NeDokumen38 halaman[International Endodontic Journal 2017-Jul 26 Vol. 51] Nazzal, H_ Kenny, K_ Altimimi, A_ Kang, J_ Duggal, M S - A Prospective Clinical Study of Regenerative Endodontic Treatment of Traumatised Immature Teeth With Neكرم الباريBelum ada peringkat
- Comparative Desensitizing Effect of A Toothpaste and Mouthwash (Potassium Nitrate)Dokumen7 halamanComparative Desensitizing Effect of A Toothpaste and Mouthwash (Potassium Nitrate)AsriDianSariBelum ada peringkat
- Preventive Effect of An Orthodontic Compomer Against Enamel Demineralization Around Bonded BracketsDokumen5 halamanPreventive Effect of An Orthodontic Compomer Against Enamel Demineralization Around Bonded BracketsAsep J PermanaBelum ada peringkat
- Deber 4 Art 3Dokumen11 halamanDeber 4 Art 3Mile MolinaBelum ada peringkat
- Dentoalveolar Trauma: Ted Fields, DDSDokumen26 halamanDentoalveolar Trauma: Ted Fields, DDSCak BasitBelum ada peringkat
- Peri-Implant Complications: A Clinical Guide to Diagnosis and TreatmentDari EverandPeri-Implant Complications: A Clinical Guide to Diagnosis and TreatmentBelum ada peringkat
- الأب الغني والأب الفقيرDokumen244 halamanالأب الغني والأب الفقيرKhalid G. AzouniBelum ada peringkat
- Guidelines For Periodontal Therapy - CoggleDokumen1 halamanGuidelines For Periodontal Therapy - CoggleKhalid G. AzouniBelum ada peringkat
- Delivering Better Oral Health Evidence-Based GuidanceDokumen4 halamanDelivering Better Oral Health Evidence-Based GuidanceKhalid G. AzouniBelum ada peringkat
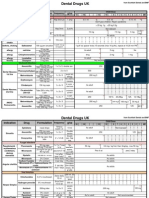
- ORE DrugsDokumen4 halamanORE DrugsKhalid G. AzouniBelum ada peringkat
- Postoperative Sensitivity in Direct Resin CompositesDokumen12 halamanPostoperative Sensitivity in Direct Resin CompositesKhalid G. AzouniBelum ada peringkat
- Endodontics in The Modern Era FINALDokumen4 halamanEndodontics in The Modern Era FINALKhalid G. AzouniBelum ada peringkat
- The Correct QiblaDokumen36 halamanThe Correct Qiblandaru_adyonoBelum ada peringkat
- Kelk TutDokumen12 halamanKelk TutJawaadAliBelum ada peringkat
- CDC Guidelines DisinfectionDokumen158 halamanCDC Guidelines DisinfectionamomentcastingBelum ada peringkat
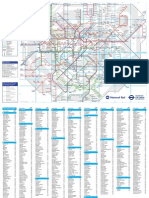
- London Rail and Tube Services MapDokumen2 halamanLondon Rail and Tube Services MapKhalid G. AzouniBelum ada peringkat
- Basic Properties of Dental MaterialsDokumen14 halamanBasic Properties of Dental MaterialsEva FebrinaBelum ada peringkat
- Dental CariesDokumen15 halamanDental CariesImran KhanBelum ada peringkat
- TRP-C5 Sensor Odontoblastos FrioDokumen13 halamanTRP-C5 Sensor Odontoblastos FrioIgna Sarquis AbumohorBelum ada peringkat
- Enamel, Dentin, Pulp Biological ConsiderationDokumen41 halamanEnamel, Dentin, Pulp Biological ConsiderationMohammad ABelum ada peringkat
- 01 Dentin and PulpDokumen135 halaman01 Dentin and PulpMinh NguyenBelum ada peringkat
- Cobourne (1999) The Genetic Control of Early OdontogenesisDokumen0 halamanCobourne (1999) The Genetic Control of Early OdontogenesisMaja Maja BułkaBelum ada peringkat
- Tooth Root FormationDokumen10 halamanTooth Root FormationAthenaeum Scientific PublishersBelum ada peringkat
- Krok 1 Stomatology: Test Items For Licensing ExaminationDokumen28 halamanKrok 1 Stomatology: Test Items For Licensing ExaminationhelloBelum ada peringkat
- NEET MDS Picture Based QuestionsDokumen74 halamanNEET MDS Picture Based QuestionsAysha NazrinBelum ada peringkat
- Dental PulpDokumen112 halamanDental PulpLuciano AbbaBelum ada peringkat
- Selective Caries ExcavationDokumen10 halamanSelective Caries Excavationjorefe12Belum ada peringkat
- Histology of Tooth DevelopmentDokumen31 halamanHistology of Tooth DevelopmentMuzzamil MughalBelum ada peringkat
- Ten Cates Oral Histology Development Structure and Function 9th Edition Ebook PDF VersionDokumen62 halamanTen Cates Oral Histology Development Structure and Function 9th Edition Ebook PDF Versiondaniel.salazar67898% (40)
- Calcium Hydroxide Induced Resorption of Deciduous Teeth A Possible ExplanationDokumen6 halamanCalcium Hydroxide Induced Resorption of Deciduous Teeth A Possible ExplanationRishabh KapoorBelum ada peringkat
- The General Anatomy of The Teeth Comparative Anatomy of The TeethDokumen9 halamanThe General Anatomy of The Teeth Comparative Anatomy of The Teethsomebody_maBelum ada peringkat
- Preserving Pulp VitalityDokumen2 halamanPreserving Pulp VitalitygsaveitBelum ada peringkat
- Japanese Dental Science Review: Jorge PerdigãoDokumen8 halamanJapanese Dental Science Review: Jorge PerdigãoJAIR DIEGO VIDAURRE QUISPEBelum ada peringkat
- Pathogenesis of Pulpitis Resulting From Dental CariesDokumen9 halamanPathogenesis of Pulpitis Resulting From Dental CariesErnestoBelum ada peringkat
- Pulpotomies For Primary Teeth July 2010Dokumen59 halamanPulpotomies For Primary Teeth July 2010Raksmey PhanBelum ada peringkat
- Stages of Tooth DevelopmentDokumen6 halamanStages of Tooth DevelopmentSOUMYA A DR, DEPT.OF DENTAL SCIENCES,SRIHERBelum ada peringkat
- Dentinogenesis: Dr. Asmat Jameel Assistant Professor B.D.S, F.C.P.S Head Department of Oral BiologyDokumen17 halamanDentinogenesis: Dr. Asmat Jameel Assistant Professor B.D.S, F.C.P.S Head Department of Oral Biologylisa chanBelum ada peringkat
- Amelogenin Phosphorylation Regulates Tooth Enamel Formation by Stabilizing A Transient Amorphous Mineral PrecursorDokumen17 halamanAmelogenin Phosphorylation Regulates Tooth Enamel Formation by Stabilizing A Transient Amorphous Mineral PrecursorratrikaruniaBelum ada peringkat
- Management of Deep Caries 1st PartDokumen45 halamanManagement of Deep Caries 1st PartLames Ali Sayed Ahmed AttiaBelum ada peringkat
- Dental Pulp: University of Djilali Liables Faculty of Medecine Taleb Mourad Departement of DentistryDokumen42 halamanDental Pulp: University of Djilali Liables Faculty of Medecine Taleb Mourad Departement of DentistryjoumanaBelum ada peringkat
- EnamelDokumen11 halamanEnamel3ezzat100% (1)
































































![[International Endodontic Journal 2017-Jul 26 Vol. 51] Nazzal, H_ Kenny, K_ Altimimi, A_ Kang, J_ Duggal, M S - A Prospective Clinical Study of Regenerative Endodontic Treatment of Traumatised Immature Teeth With Ne](https://imgv2-2-f.scribdassets.com/img/document/649306081/149x198/6cdc9cdd33/1685435519?v=1)