Anda mungkin juga menyukai
- Complications During and After Cataract Surgery: A Guide to Surgical ManagementDari EverandComplications During and After Cataract Surgery: A Guide to Surgical ManagementBelum ada peringkat
- Allround ExDokumen1 halamanAllround ExOpl UhkBelum ada peringkat
- Como Criar Frases CromáticasDokumen2 halamanComo Criar Frases CromáticasMoisesBelum ada peringkat
- Canine Sternum and RibDokumen3 halamanCanine Sternum and RibcharlieBelum ada peringkat
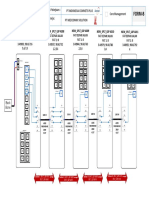
- Visio-Flowcore Feeder Milala 2Dokumen3 halamanVisio-Flowcore Feeder Milala 2Indah SyafaniBelum ada peringkat
- Visio-Flowcore Feeder Milala 2Dokumen3 halamanVisio-Flowcore Feeder Milala 2Indah SyafaniBelum ada peringkat
- Guitar Riffs: 120 Day TripperDokumen1 halamanGuitar Riffs: 120 Day TripperSteven SwiftBelum ada peringkat
- BFS and DFSDokumen9 halamanBFS and DFSLeela PallavaBelum ada peringkat
- Frogs Phylum: Chordata Subphylum: Vertebrata Class: Amphibia Order: Anura ( Salientia) Family: Ranidae Genus: 6 8Dokumen2 halamanFrogs Phylum: Chordata Subphylum: Vertebrata Class: Amphibia Order: Anura ( Salientia) Family: Ranidae Genus: 6 8Kamille PobleteBelum ada peringkat
- Family Star Plus User Guide Preview PDFDokumen17 halamanFamily Star Plus User Guide Preview PDFSimona TonciuBelum ada peringkat
- Hydrodynamic Measurements FormatDokumen3 halamanHydrodynamic Measurements FormatRenzo ChavezBelum ada peringkat
- Laporan FSE Andrian MayDokumen27 halamanLaporan FSE Andrian MayAndre PrimaBelum ada peringkat
- NAQDOWN PowerpointDokumen55 halamanNAQDOWN PowerpointsarahbeeBelum ada peringkat
- Patient IV fluid intake record templateDokumen1 halamanPatient IV fluid intake record templatemarcelinaBelum ada peringkat
- Back To School Color by NumberDokumen3 halamanBack To School Color by NumberRalph CharlesBelum ada peringkat
- SLASH Warm Up Exercise PDFDokumen1 halamanSLASH Warm Up Exercise PDFRonaldo OrtizBelum ada peringkat
- Warm up exercise in half step down tuningDokumen1 halamanWarm up exercise in half step down tuningIncredible MaxBelum ada peringkat
- Faster By The Day Program Week 4Dokumen1 halamanFaster By The Day Program Week 4RegeTrolleXBelum ada peringkat
- Augmented Chord ShapesDokumen2 halamanAugmented Chord ShapesSteven SwiftBelum ada peringkat
- Statistical Meeting 19 MayDokumen3 halamanStatistical Meeting 19 MayRahul ThakurBelum ada peringkat
- Musical (5 e 10 Minutos) : Exercicio 3 (Diagonal) Kiko Loureiro Guitar WorkoutDokumen1 halamanMusical (5 e 10 Minutos) : Exercicio 3 (Diagonal) Kiko Loureiro Guitar WorkoutArthur MonteiroBelum ada peringkat
- Musical (5 e 10 Minutos) : Exercicio 4 (Diagonal Com Saltos) Kiko Loureiro Guitar WorkoutDokumen1 halamanMusical (5 e 10 Minutos) : Exercicio 4 (Diagonal Com Saltos) Kiko Loureiro Guitar WorkoutArthur MonteiroBelum ada peringkat
- Design City ValheimDokumen1 halamanDesign City Valheimnick.gsimonBelum ada peringkat
- Environmental Impact Matrix AnalysisDokumen15 halamanEnvironmental Impact Matrix AnalysisdebryaniBelum ada peringkat
- Wmuji 006Dokumen4 halamanWmuji 006li LewisBelum ada peringkat
- Dashboard Data: Safety Inspections Safety Walkthroughs Hazard HuntsDokumen4 halamanDashboard Data: Safety Inspections Safety Walkthroughs Hazard HuntsWilson Lozano SilvaBelum ada peringkat
- ExcelDokumen9 halamanExcelBharath BuddyBelum ada peringkat
- Angèle - Balance Ton Quoi (Guitar 1)Dokumen1 halamanAngèle - Balance Ton Quoi (Guitar 1)Leander LyonsBelum ada peringkat
- Typhoon Preparedness Checklist Huni Lio May 25, 2023Dokumen2 halamanTyphoon Preparedness Checklist Huni Lio May 25, 2023jordan calderonBelum ada peringkat
- Fetal Biometry and Growth ChartsDokumen27 halamanFetal Biometry and Growth ChartsnellieauthorBelum ada peringkat
- LoopPlay Façon ThunderstruckDokumen1 halamanLoopPlay Façon ThunderstruckwoalithBelum ada peringkat
- Sotto 'O SoleDokumen5 halamanSotto 'O SoleFabrice PieriBelum ada peringkat
- Captura de Tela 2023-05-22 À(s) 14.54.10Dokumen8 halamanCaptura de Tela 2023-05-22 À(s) 14.54.10Felipe SilveiraBelum ada peringkat
- Arpeggios PhrygianDokumen1 halamanArpeggios PhrygianMarcelo KimuraBelum ada peringkat
- VINARES Booklet V008Dokumen21 halamanVINARES Booklet V008Imadh NāsirBelum ada peringkat
- Jazz Blues Etude: PerformanceDokumen3 halamanJazz Blues Etude: PerformanceThuy Tien Nguyen Hoang100% (1)
- I Will SurviveDokumen9 halamanI Will SurviveClavileño El AlígeroBelum ada peringkat
- Just The Two of Us FminDokumen1 halamanJust The Two of Us FminSébastien AndreBelum ada peringkat
- I Care Leader Summary ReportDokumen1 halamanI Care Leader Summary ReportAgus Rohmad NurhidayahBelum ada peringkat
- Major II V I LinesDokumen1 halamanMajor II V I LinesPete Sklaroff100% (1)
- Forensic identification techniques of Nueva Ecija UniversityDokumen3 halamanForensic identification techniques of Nueva Ecija UniversitySean R BnBelum ada peringkat
- Behavior tracking sheetDokumen2 halamanBehavior tracking sheetrobin luoBelum ada peringkat
- Bad Intent (Solo) - Frank Gambale - Concert With ClassDokumen6 halamanBad Intent (Solo) - Frank Gambale - Concert With ClassKurtis LeCompteBelum ada peringkat
- So Easy, So EffectiveDokumen1 halamanSo Easy, So EffectiveFerdinand SiahaanBelum ada peringkat
- Strong Room DWG-ModelDokumen1 halamanStrong Room DWG-ModelDelight Survey consultancyBelum ada peringkat
- Constipation IN OLD AGEDokumen49 halamanConstipation IN OLD AGEbrightagbotuiBelum ada peringkat
- O'clock O'clock O'clock: A M P M P MDokumen20 halamanO'clock O'clock O'clock: A M P M P Msandeep_walia1499Belum ada peringkat
- JoJo's Bizarre Adventure Stone Ocean OP Bass TabDokumen3 halamanJoJo's Bizarre Adventure Stone Ocean OP Bass Tabelliotiguer199Belum ada peringkat
- Forgotten PalestiniansDokumen345 halamanForgotten Palestinianscacing ghoibBelum ada peringkat
- EstrellitaDokumen1 halamanEstrellitaungatofachero2Belum ada peringkat
- Tefb 018 PDFDokumen2 halamanTefb 018 PDFJASWANTH K PBelum ada peringkat
- HL740 6-4Dokumen23 halamanHL740 6-4REMZONABelum ada peringkat
- Apollo Hospital International Limited: Nirali S.Donga A-One Pharmacy College (1 September, 2020 To 27 September, 2020)Dokumen7 halamanApollo Hospital International Limited: Nirali S.Donga A-One Pharmacy College (1 September, 2020 To 27 September, 2020)Nirali DongaBelum ada peringkat
- Nr. Matricserie Grupa Credit Punctaj Media RadiologradiologDokumen3 halamanNr. Matricserie Grupa Credit Punctaj Media RadiologradiologAlexandra EnacheBelum ada peringkat
- PPMC November 2023-WorkbookDokumen40 halamanPPMC November 2023-Workbookanil sharmaBelum ada peringkat
- 5 Pentatonic IDEASDokumen2 halaman5 Pentatonic IDEASMaksym BohorodichenkoBelum ada peringkat
- The 1975's Somebody Else Sheet MusicDokumen7 halamanThe 1975's Somebody Else Sheet MusicLuis Fernando Ore PericanazasBelum ada peringkat
- The 1975 Song Somebody Else LyricsDokumen7 halamanThe 1975 Song Somebody Else LyricsLuis Fernando Ore PericanazasBelum ada peringkat
- Message in A Bottle (2) : Machine HeadDokumen3 halamanMessage in A Bottle (2) : Machine HeadRichard Estid Borja QuirozBelum ada peringkat
- Current Management of LabourDokumen48 halamanCurrent Management of Labourapi-3705046100% (4)
- Abdominal Pain in PregnancyDokumen22 halamanAbdominal Pain in Pregnancyapi-3705046Belum ada peringkat
- Dysfunctional Uterine Bleeding (DUB)Dokumen21 halamanDysfunctional Uterine Bleeding (DUB)api-3705046100% (2)
- Ovarian TumoursDokumen17 halamanOvarian Tumoursapi-3705046100% (3)
- Detrusor InstabilityDokumen7 halamanDetrusor Instabilityapi-3705046Belum ada peringkat
- Weight Gain in PregnancyDokumen18 halamanWeight Gain in Pregnancyapi-3705046Belum ada peringkat
- House OfficerDokumen32 halamanHouse Officerapi-3705046100% (1)
- Cervical Incompetence 1Dokumen5 halamanCervical Incompetence 1api-3705046100% (1)
- VVF Clinical Presentation 1Dokumen24 halamanVVF Clinical Presentation 1api-370504683% (6)
- ContraceptionDokumen39 halamanContraceptionapi-3705046100% (3)
- HODokumen14 halamanHOapi-3705046Belum ada peringkat
- House OfficerDokumen32 halamanHouse Officerapi-3705046100% (1)
- Vulvar MalignancyDokumen21 halamanVulvar Malignancyapi-3705046Belum ada peringkat
- Uterine FibroidsDokumen11 halamanUterine Fibroidsapi-3705046Belum ada peringkat
- Vaginal Birth After Caesarean Section (Vbac)Dokumen16 halamanVaginal Birth After Caesarean Section (Vbac)api-370504650% (2)
- Uterovaginal ProlapseDokumen16 halamanUterovaginal Prolapseapi-3705046100% (1)
- Reprodctive HealthDokumen4 halamanReprodctive Healthapi-3705046Belum ada peringkat
- Vesico Vaginal FistulaDokumen6 halamanVesico Vaginal Fistulaapi-3705046Belum ada peringkat
- The Incompetent Cervix 1Dokumen10 halamanThe Incompetent Cervix 1api-3705046100% (1)
- Thyroid Diseases in PregnancyDokumen18 halamanThyroid Diseases in Pregnancyapi-3705046100% (3)
- Unstable LieDokumen7 halamanUnstable Lieapi-370504667% (3)
- Rhesus Iso ImmunizationDokumen12 halamanRhesus Iso Immunizationapi-3705046Belum ada peringkat
- Renal Disease in PregDokumen22 halamanRenal Disease in Pregapi-3705046100% (1)
- The Incompetent Cervix 2Dokumen30 halamanThe Incompetent Cervix 2api-3705046100% (3)
- Sickle Cell Disease in PregnancyDokumen18 halamanSickle Cell Disease in Pregnancyapi-370504667% (3)
- Roll Back MalariaDokumen2 halamanRoll Back Malariaapi-3705046Belum ada peringkat
- Septic AbortionDokumen15 halamanSeptic Abortionapi-3705046Belum ada peringkat
- PubertyDokumen7 halamanPubertyapi-3705046Belum ada peringkat
- Preeclampsia and EclampsiaDokumen23 halamanPreeclampsia and Eclampsiaapi-3705046100% (6)
- Preterm Rupture of Foetal MembranesDokumen24 halamanPreterm Rupture of Foetal Membranesapi-3705046Belum ada peringkat
- Container sizes: 20', 40' dimensions and specificationsDokumen3 halamanContainer sizes: 20', 40' dimensions and specificationsStylefasBelum ada peringkat
- Principles of DisplaysDokumen2 halamanPrinciples of DisplaysShamanthakBelum ada peringkat
- INDEX OF 3D PRINTED CONCRETE RESEARCH DOCUMENTDokumen15 halamanINDEX OF 3D PRINTED CONCRETE RESEARCH DOCUMENTAkhwari W. PamungkasjatiBelum ada peringkat
- Kristine Karen DavilaDokumen3 halamanKristine Karen DavilaMark anthony GironellaBelum ada peringkat
- CSEC Geography June 2014 P1Dokumen14 halamanCSEC Geography June 2014 P1Josh Hassanali100% (1)
- Extra Vocabulary: Extension Units 1 & 2Dokumen1 halamanExtra Vocabulary: Extension Units 1 & 2CeciBravoBelum ada peringkat
- Walter Horatio Pater (4 August 1839 - 30 July 1894) Was An English EssayistDokumen4 halamanWalter Horatio Pater (4 August 1839 - 30 July 1894) Was An English EssayistwiweksharmaBelum ada peringkat
- Factors Affecting Job Satisfaction of EngineersDokumen35 halamanFactors Affecting Job Satisfaction of Engineerslingg8850% (2)
- TCW The Global CityDokumen40 halamanTCW The Global CityAllen Carl100% (1)
- CV Finance GraduateDokumen3 halamanCV Finance GraduateKhalid SalimBelum ada peringkat
- String length recommendations and brace height advice for Uukha bowsDokumen1 halamanString length recommendations and brace height advice for Uukha bowsPak Cik FauzyBelum ada peringkat
- First Time Login Guidelines in CRMDokumen23 halamanFirst Time Login Guidelines in CRMSumeet KotakBelum ada peringkat
- Classwork Notes and Pointers Statutory Construction - TABORDA, CHRISTINE ANNDokumen47 halamanClasswork Notes and Pointers Statutory Construction - TABORDA, CHRISTINE ANNChristine Ann TabordaBelum ada peringkat
- 2nd YearDokumen5 halaman2nd YearAnbalagan GBelum ada peringkat
- RFID Sticker and and Card Replacement 2019 PDFDokumen1 halamanRFID Sticker and and Card Replacement 2019 PDFJessamyn DimalibotBelum ada peringkat
- Felomino Urbano vs. IAC, G.R. No. 72964, January 7, 1988 ( (157 SCRA 7)Dokumen1 halamanFelomino Urbano vs. IAC, G.R. No. 72964, January 7, 1988 ( (157 SCRA 7)Dwight LoBelum ada peringkat
- 100 Bedded Hospital at Jadcherla: Load CalculationsDokumen3 halaman100 Bedded Hospital at Jadcherla: Load Calculationskiran raghukiranBelum ada peringkat
- Miss Daydreame1Dokumen1 halamanMiss Daydreame1Mary Joy AlbandiaBelum ada peringkat
- Polisomnografí A Dinamica No Dise.: Club de Revistas Julián David Cáceres O. OtorrinolaringologíaDokumen25 halamanPolisomnografí A Dinamica No Dise.: Club de Revistas Julián David Cáceres O. OtorrinolaringologíaDavid CáceresBelum ada peringkat
- Other Project Content-1 To 8Dokumen8 halamanOther Project Content-1 To 8Amit PasiBelum ada peringkat
- Theories of LeadershipDokumen24 halamanTheories of Leadershipsija-ekBelum ada peringkat
- Puberty and The Tanner StagesDokumen2 halamanPuberty and The Tanner StagesPramedicaPerdanaPutraBelum ada peringkat
- FS2 Learning Experience 1Dokumen11 halamanFS2 Learning Experience 1Jona May BastidaBelum ada peringkat
- Human Resource Development's Evaluation in Public ManagementDokumen9 halamanHuman Resource Development's Evaluation in Public ManagementKelas KP LAN 2018Belum ada peringkat
- Practical Research 1 - Quarter 1 - Module 1 - Nature and Inquiry of Research - Version 3Dokumen53 halamanPractical Research 1 - Quarter 1 - Module 1 - Nature and Inquiry of Research - Version 3Iris Rivera-PerezBelum ada peringkat
- Preterm Labour: Muhammad Hanif Final Year MBBSDokumen32 halamanPreterm Labour: Muhammad Hanif Final Year MBBSArslan HassanBelum ada peringkat
- MES - Project Orientation For Night Study - V4Dokumen41 halamanMES - Project Orientation For Night Study - V4Andi YusmarBelum ada peringkat
- Decision Support System for Online ScholarshipDokumen3 halamanDecision Support System for Online ScholarshipRONALD RIVERABelum ada peringkat
- 2-Library - IJLSR - Information - SumanDokumen10 halaman2-Library - IJLSR - Information - SumanTJPRC PublicationsBelum ada peringkat
- School of Architecture, Building and Design Foundation in Natural Build EnvironmentDokumen33 halamanSchool of Architecture, Building and Design Foundation in Natural Build Environmentapi-291031287Belum ada peringkat