Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Nursing Care Plan For Impaired Comfort NCPDokumen2 halamanNursing Care Plan For Impaired Comfort NCPderic82% (11)
- 1990-Fleming Suturing Method and PainDokumen7 halaman1990-Fleming Suturing Method and PainAnonymous bq4KY0mcWG0% (1)
- The Problem of Anabiosis or Latent LifeDokumen44 halamanThe Problem of Anabiosis or Latent LifeAlexander ChurchillBelum ada peringkat
- Laporan Total Penjualan Per Barang Februari Ps PDFDokumen25 halamanLaporan Total Penjualan Per Barang Februari Ps PDFSerlyin MonicaBelum ada peringkat
- Brosur Intensa GoDokumen8 halamanBrosur Intensa GoAnonymous tbJ24554Belum ada peringkat
- A Seminar Report ON Blue BrainDokumen20 halamanA Seminar Report ON Blue BrainAngela KaifBelum ada peringkat
- Ice TherapyDokumen5 halamanIce TherapyDiane CastillonBelum ada peringkat
- Airvo 2 User Manual Ui 185045495 FDokumen76 halamanAirvo 2 User Manual Ui 185045495 Fdnavarro0050% (2)
- Bio1301 Lecture Note - Plant Section PDFDokumen32 halamanBio1301 Lecture Note - Plant Section PDFAjomBelum ada peringkat
- Juvenile HormoneDokumen17 halamanJuvenile HormonejugesmangangBelum ada peringkat
- CellBiologyLec3Spring2020DrMIKotbEl SayedDokumen35 halamanCellBiologyLec3Spring2020DrMIKotbEl SayeddeyanBelum ada peringkat
- Chap17-Program Design For Resistance TrainingDokumen46 halamanChap17-Program Design For Resistance TrainingPaulo CameloBelum ada peringkat
- Lecture 3 Cell Cycle - QuestionsDokumen6 halamanLecture 3 Cell Cycle - Questions中华雅思王Belum ada peringkat
- NullDokumen6 halamanNullapi-24723002Belum ada peringkat
- Rev Notes Ch06 eDokumen9 halamanRev Notes Ch06 eCHIU KEUNG OFFICIAL PROBelum ada peringkat
- Acute Complication of DM: Clinical Manifestation Laboratory Procedures Therapeutic Plan Possible Problem AssociatedDokumen12 halamanAcute Complication of DM: Clinical Manifestation Laboratory Procedures Therapeutic Plan Possible Problem AssociatedironBelum ada peringkat
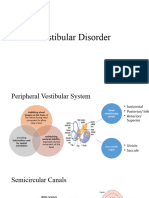
- Vestibular DisorderDokumen22 halamanVestibular DisorderSumbal SalikBelum ada peringkat
- CPRDokumen24 halamanCPRNat YueBelum ada peringkat
- Acid - Base BalanceDokumen13 halamanAcid - Base Balanceadam yassineBelum ada peringkat
- Experiment No.9Dokumen7 halamanExperiment No.9ZethBlancada Diesta BarramedaBelum ada peringkat
- The Structure and Function of The BrainDokumen25 halamanThe Structure and Function of The BrainNo NameBelum ada peringkat
- Prep, Dressing, Draping The PatientDokumen60 halamanPrep, Dressing, Draping The PatientTamil Villardo100% (1)
- CarbohydratesDokumen6 halamanCarbohydratesNarasimha MurthyBelum ada peringkat
- Science Form 2 - Chapter 1Dokumen46 halamanScience Form 2 - Chapter 1Mohamad TarmiziBelum ada peringkat
- Activity 1.5cell DivisionDokumen2 halamanActivity 1.5cell Divisionfroilan obligadoBelum ada peringkat
- FertilityDokumen207 halamanFertilitypmotcBelum ada peringkat
- Bio PP1 QS Pre-Mock 2024.Dokumen9 halamanBio PP1 QS Pre-Mock 2024.Elvis KemboiBelum ada peringkat
- WORKSHOP No 3Dokumen20 halamanWORKSHOP No 3Yainel RomeroBelum ada peringkat
- Scientific Classification: CladeDokumen3 halamanScientific Classification: Clademarijana_zBelum ada peringkat
- (Ih Lec) 1ST ShiftDokumen73 halaman(Ih Lec) 1ST ShiftDennisse San JoseBelum ada peringkat