Anda mungkin juga menyukai
- CYSTOCLYSISDokumen1 halamanCYSTOCLYSISzerpthederpBelum ada peringkat
- Rheumatic Heart DiseaseDokumen5 halamanRheumatic Heart DiseasezerpthederpBelum ada peringkat
- Grand Case Study 2Dokumen2 halamanGrand Case Study 2zerpthederpBelum ada peringkat
- Psychiatric Nursing Bullets (Nle & Nclex)Dokumen21 halamanPsychiatric Nursing Bullets (Nle & Nclex)Richard Ines Valino100% (24)
- Requirements For Perpetual Succour Hospital PGNTDokumen1 halamanRequirements For Perpetual Succour Hospital PGNTzerpthederpBelum ada peringkat
- Session 4: Main SymptomsDokumen86 halamanSession 4: Main SymptomszerpthederpBelum ada peringkat
- Drug StudyDokumen3 halamanDrug Studyudntnid2knwme100% (4)
- Feature StoriesDokumen1 halamanFeature StorieszerpthederpBelum ada peringkat
- Case Study of A Patient With Ischemic CardiomyopathyDokumen33 halamanCase Study of A Patient With Ischemic Cardiomyopathyromeo rivera80% (5)
- Drusadg Study For Paracetamol Omeprazole and Vitamin B ComplexDokumen3 halamanDrusadg Study For Paracetamol Omeprazole and Vitamin B ComplexzerpthederpBelum ada peringkat
- Compilation OF Case Studies: Perpetual Succour Hospital Gorordo Ave., Lahug, Cebu City Nursing Service DepartmentDokumen1 halamanCompilation OF Case Studies: Perpetual Succour Hospital Gorordo Ave., Lahug, Cebu City Nursing Service DepartmentzerpthederpBelum ada peringkat
- Grand Cassade Study 1Dokumen15 halamanGrand Cassade Study 1zerpthederpBelum ada peringkat
- Foetal CirculationDokumen8 halamanFoetal CirculationMujahid_Dean_8976Belum ada peringkat
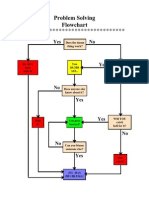
- Problem Solving Flowchart: Yes NoDokumen1 halamanProblem Solving Flowchart: Yes NozerpthederpBelum ada peringkat
- When in Rome PDFDokumen120 halamanWhen in Rome PDFzerpthederpBelum ada peringkat
- Identifying Our Own ProblemsDokumen8 halamanIdentifying Our Own ProblemszerpthederpBelum ada peringkat
- CokeDokumen3 halamanCokezerpthederpBelum ada peringkat
- Community Needs AssessmentDokumen13 halamanCommunity Needs Assessmentzerpthederp0% (1)
- 12 Literary Compositions That Have Influenced The WorldDokumen3 halaman12 Literary Compositions That Have Influenced The Worldzerpthederp100% (6)
- Welcome AddressDokumen1 halamanWelcome AddresszerpthederpBelum ada peringkat
- Bohol SUPREME STUDENT GOV'T Liquidation ReportDokumen1 halamanBohol SUPREME STUDENT GOV'T Liquidation ReportzerpthederpBelum ada peringkat
- NMAT ID Form-1111302389Dokumen1 halamanNMAT ID Form-1111302389zerpthederpBelum ada peringkat
- UlcerDokumen3 halamanUlcerAjay SathyanBelum ada peringkat
- UBCN Nursing Event SponsorshipDokumen3 halamanUBCN Nursing Event SponsorshipzerpthederpBelum ada peringkat
- TOPICDokumen1 halamanTOPICzerpthederpBelum ada peringkat
- UBCN Nursing Staff Event SponsorshipDokumen2 halamanUBCN Nursing Staff Event SponsorshipzerpthederpBelum ada peringkat
- CIM Application Form 1Dokumen1 halamanCIM Application Form 1Kara AguilarBelum ada peringkat
- Dengue Fever Case StudyDokumen24 halamanDengue Fever Case Studymaemaeyee95% (22)
- Session 4: Main SymptomsDokumen86 halamanSession 4: Main SymptomszerpthederpBelum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Loan PredictionDokumen3 halamanLoan PredictionShreyansh JainBelum ada peringkat
- Problem Set 1 CirclesDokumen2 halamanProblem Set 1 Circlesapi-339611548100% (1)
- TRL External CommunicationDokumen3 halamanTRL External CommunicationAyushGargBelum ada peringkat
- MC0081Dokumen385 halamanMC0081Purushottam KumarBelum ada peringkat
- Catalogo Carbones Helwig GDE-006Dokumen17 halamanCatalogo Carbones Helwig GDE-006Sergio HernandezBelum ada peringkat
- WCS1400 / WCS1400S: FeaturesDokumen7 halamanWCS1400 / WCS1400S: FeaturesbahrowiadiBelum ada peringkat
- Science8 Q2 Module3 (Week6)Dokumen30 halamanScience8 Q2 Module3 (Week6)Mary Grace Lemon100% (1)
- Hargreaves 2007Dokumen15 halamanHargreaves 2007Sam GonçalvesBelum ada peringkat
- Ductile deformation finite strain analysisDokumen27 halamanDuctile deformation finite strain analysisJorgeBarriosMurielBelum ada peringkat
- Is 14416 1996Dokumen20 halamanIs 14416 1996kaustavBelum ada peringkat
- Eng Grammar Book 8Dokumen77 halamanEng Grammar Book 8ЖАНСАЯ Сейдахмет50% (2)
- Manuscript 123Dokumen46 halamanManuscript 123Datuzuharto Sultan100% (1)
- Hospital Managemen T System: Oose LAB FileDokumen62 halamanHospital Managemen T System: Oose LAB FileAASHBelum ada peringkat
- 9 CE AmplifierDokumen5 halaman9 CE AmplifierAnsh PratapBelum ada peringkat
- Fiziks: Basic Properties and Tools of ThermodynamicsDokumen28 halamanFiziks: Basic Properties and Tools of ThermodynamicsSURAJ PRATAP SINGHBelum ada peringkat
- Formulas For Thermodynamics 1Dokumen2 halamanFormulas For Thermodynamics 1Stefani Ann CabalzaBelum ada peringkat
- Testing of Semifinished Products of Thermoplastics Bases - Indications Directive DVS 2201-1Dokumen4 halamanTesting of Semifinished Products of Thermoplastics Bases - Indications Directive DVS 2201-1OscarBelum ada peringkat
- Unit 6 - Quantitative Analysis NotesDokumen53 halamanUnit 6 - Quantitative Analysis Notesapi-182809945Belum ada peringkat
- QAP - LT Panel PDFDokumen8 halamanQAP - LT Panel PDFAkshay Ajay100% (2)
- Daikin RXS-K - Technical DataDokumen21 halamanDaikin RXS-K - Technical DataPrestoneKBelum ada peringkat
- Composition, Thermal and Rheological Behaviour of Selected Greek HoneysDokumen13 halamanComposition, Thermal and Rheological Behaviour of Selected Greek HoneyssyazaqilahBelum ada peringkat
- Signal Circuit LessonDokumen1 halamanSignal Circuit Lessonapi-208557858Belum ada peringkat
- Wound ScaleDokumen4 halamanWound ScaleHumam SyriaBelum ada peringkat
- Chapter 1: Introduction: 1.1 Background TheoryDokumen36 halamanChapter 1: Introduction: 1.1 Background TheoryBe-fit Be-strongBelum ada peringkat
- Methodology of Event StudiesDokumen4 halamanMethodology of Event Studieshaichellam5577Belum ada peringkat
- CSEC-Chemistry-p2 May-June 2012 PDFDokumen20 halamanCSEC-Chemistry-p2 May-June 2012 PDFdela250% (4)
- Final Project Regenerative BrakingDokumen6 halamanFinal Project Regenerative Brakingdims irifiyinBelum ada peringkat
- Woodward MFR 13Dokumen91 halamanWoodward MFR 13OryaBelum ada peringkat
- AC axial compact fan technical specificationsDokumen5 halamanAC axial compact fan technical specificationsdhanasekhar27Belum ada peringkat
- Er DiagramsDokumen20 halamanEr DiagramsMatthew BloomfieldBelum ada peringkat