Anda mungkin juga menyukai
- Tanner StagesDokumen2 halamanTanner Stagesratnaupiq100% (1)
- Clinical Evaluation Report-Surgical InstrumentsDokumen8 halamanClinical Evaluation Report-Surgical InstrumentsAlejandro Landinez0% (1)
- Anorectal MalformationsDokumen28 halamanAnorectal MalformationsVisu ReddyBelum ada peringkat
- Abnormalities Of The Testis And Scrotum: A Concise GuideDokumen34 halamanAbnormalities Of The Testis And Scrotum: A Concise GuideIma MoriBelum ada peringkat
- (2017) OGUNYEMI, Boluwaji MILLER-MONTHROPE, Yvette. The State of Ethnic Dermatology in CanadaDokumen3 halaman(2017) OGUNYEMI, Boluwaji MILLER-MONTHROPE, Yvette. The State of Ethnic Dermatology in CanadaCassandra VérasBelum ada peringkat
- Nursing Care Plan: Interaction Immediate Cause Goal: Effectivenes SDokumen6 halamanNursing Care Plan: Interaction Immediate Cause Goal: Effectivenes SCatherine Kaye Marquez RoxasBelum ada peringkat
- Organizing Nursing Service and Patient CareDokumen32 halamanOrganizing Nursing Service and Patient CareGrashia100% (2)
- Exstrophy and Epispadias MedscapeDokumen18 halamanExstrophy and Epispadias MedscapeMohammad Rifqi WibowoBelum ada peringkat
- Imperforate Anus and Cloacal MalformationsDokumen110 halamanImperforate Anus and Cloacal MalformationsAhmad Abu KushBelum ada peringkat
- Epispadias: Causes, Symptoms and TreatmentDokumen22 halamanEpispadias: Causes, Symptoms and TreatmentLuthfan Dio Satria BachriBelum ada peringkat
- Management of EpispadiasDokumen12 halamanManagement of EpispadiasAlip WildanBelum ada peringkat
- HipospadiDokumen12 halamanHipospadiArtrinda AnggitaBelum ada peringkat
- Imperforate Anus and Cloacal MalformationsDokumen23 halamanImperforate Anus and Cloacal MalformationsGwyneth JangadBelum ada peringkat
- Help Pedsurgeryafrica94Dokumen13 halamanHelp Pedsurgeryafrica94Leni LukmanBelum ada peringkat
- True Undescened TestesDokumen42 halamanTrue Undescened TestesSahirBelum ada peringkat
- AnorectalmalformationDokumen126 halamanAnorectalmalformationNinaBelum ada peringkat
- Operative Pediatric Surgery Anorectal MalformationDokumen21 halamanOperative Pediatric Surgery Anorectal MalformationZaeem KhalidBelum ada peringkat
- HypospDokumen39 halamanHypospyoussef.aziz2020Belum ada peringkat
- Anorectal Malformatio N: Dr. O. Sankoh M.D. House Officer Pediatric SurgeryDokumen123 halamanAnorectal Malformatio N: Dr. O. Sankoh M.D. House Officer Pediatric SurgeryMohamed KamaraBelum ada peringkat
- RRM's Next - Urology-Penis & UrethraDokumen32 halamanRRM's Next - Urology-Penis & UrethrairfanBelum ada peringkat
- HypopediasisDokumen8 halamanHypopediasisv_vijayakanth7656Belum ada peringkat
- EPISPADIASDokumen16 halamanEPISPADIASAmina RajahBelum ada peringkat
- Anorectal MalformationsDokumen6 halamanAnorectal Malformationskhadzx100% (2)
- Síndrome Adrenogenital e Alterações Anatômicas PDFDokumen10 halamanSíndrome Adrenogenital e Alterações Anatômicas PDFFred SilvaBelum ada peringkat
- Malformations of the genitourinary systemDokumen3 halamanMalformations of the genitourinary systemÁngel Parra CominoBelum ada peringkat
- Definition of HypospadiasDokumen3 halamanDefinition of Hypospadiasisabella fordBelum ada peringkat
- Rare Congenital Genitourinary AnomaliesDokumen27 halamanRare Congenital Genitourinary Anomaliesد. محمد عبد الباقي فهميBelum ada peringkat
- Continuing Education Activity: HypospadiasDokumen6 halamanContinuing Education Activity: HypospadiasMaulani Nurlatifah100% (1)
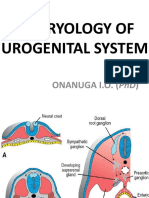
- Embryology of Urogenital SystemDokumen42 halamanEmbryology of Urogenital SystemAngetile Kasanga100% (1)
- K25 - A - Congenital Anomalies of The Urinary TractDokumen26 halamanK25 - A - Congenital Anomalies of The Urinary TractErwin SiregarBelum ada peringkat
- RenalDokumen81 halamanRenalandreaBelum ada peringkat
- Reference HipospadiaDokumen14 halamanReference HipospadiaHasya KinasihBelum ada peringkat
- Anorectal MalformationsDokumen19 halamanAnorectal MalformationsJumrotun Ni'mahBelum ada peringkat
- Anal AtresiaDokumen13 halamanAnal AtresiaAhmad IhsanBelum ada peringkat
- Congenital Anomalies of Ureter BladderDokumen17 halamanCongenital Anomalies of Ureter BladderAfiq SabriBelum ada peringkat
- Anorectal Malformations in Children - A Review: Amrish Vaidya, Kishore AdyanthayaDokumen4 halamanAnorectal Malformations in Children - A Review: Amrish Vaidya, Kishore Adyanthayasangvi_tvBelum ada peringkat
- Inguinal Hernia by Dr. TalabiDokumen16 halamanInguinal Hernia by Dr. TalabidayomanBelum ada peringkat
- A Brief Case Report of Duplicated Bladder Exstrophy A Congenital Malformation in PaediatricsDokumen3 halamanA Brief Case Report of Duplicated Bladder Exstrophy A Congenital Malformation in PaediatricsMARIA SOL MONTALVO LALALEOBelum ada peringkat
- HypospadiaDokumen21 halamanHypospadiaShi YunBelum ada peringkat
- Q Bladder L1 +2Dokumen14 halamanQ Bladder L1 +2youssef.aziz2020Belum ada peringkat
- Congenital Anomalies of Urinary BladderDokumen102 halamanCongenital Anomalies of Urinary Bladdernancy voraBelum ada peringkat
- Anorectal MalformationDokumen40 halamanAnorectal MalformationFrankBelum ada peringkat
- Malformasi AnorektalDokumen78 halamanMalformasi Anorektalusidabutar100% (2)
- Undescend Testis - OrchiopexyDokumen12 halamanUndescend Testis - Orchiopexyansar ahmedBelum ada peringkat
- Anal FistulasDokumen9 halamanAnal FistulasikeernawatiBelum ada peringkat
- Physical Examination of the Genitourinary TractDokumen12 halamanPhysical Examination of the Genitourinary TractrudybisBelum ada peringkat
- Congenital Anomalies of the Penis: Causes and Classification of HypospadiasDokumen20 halamanCongenital Anomalies of the Penis: Causes and Classification of HypospadiasMerlin MuktialiBelum ada peringkat
- Opening 1.1 BackgroundDokumen17 halamanOpening 1.1 Backgroundvictor zhefaBelum ada peringkat
- Blue Boxes For PelvisDokumen11 halamanBlue Boxes For Pelviskabal08Belum ada peringkat
- Penis: 2.1 Embryology and Penile DevelopmentDokumen27 halamanPenis: 2.1 Embryology and Penile DevelopmenteeBelum ada peringkat
- HipospadiaDokumen66 halamanHipospadiaDichaBelum ada peringkat
- Pediatric Urology HDokumen54 halamanPediatric Urology HAlaa A. AbdelrahimBelum ada peringkat
- Anorectal MalformationDokumen28 halamanAnorectal Malformationsulithkuriakose100% (2)
- Ruiz, P. - SGD and NCP On Imperforate AnusDokumen8 halamanRuiz, P. - SGD and NCP On Imperforate AnusPatricia Dianne RuizBelum ada peringkat
- Hypospadias: by Khaled Ashour John Radcliffe HsopitalDokumen87 halamanHypospadias: by Khaled Ashour John Radcliffe Hsopitalhayssam rashwanBelum ada peringkat
- Lumina.S M.SC Nursing (Child Health)Dokumen55 halamanLumina.S M.SC Nursing (Child Health)lumina.sBelum ada peringkat
- I. Objectives For Students' Independent StudiesDokumen5 halamanI. Objectives For Students' Independent StudiesFokeerbux ZyadBelum ada peringkat
- Repro CorrDokumen67 halamanRepro CorrsrhmdBelum ada peringkat
- Gambar Usg TestisDokumen28 halamanGambar Usg TestisIrfan YHBelum ada peringkat
- Congenital Abdominal Wall Defects: An IntroductionDokumen38 halamanCongenital Abdominal Wall Defects: An IntroductionAhmad Abu KushBelum ada peringkat
- Anorectal MalformationDokumen29 halamanAnorectal Malformationbimaindra97Belum ada peringkat
- Lopography Distal - MAR+fistel NizamDokumen6 halamanLopography Distal - MAR+fistel NizamMoch NizamBelum ada peringkat
- Urethral DiseaseDokumen25 halamanUrethral Diseaseyoussef.aziz2020Belum ada peringkat
- Presentation 1Dokumen2 halamanPresentation 1sheranadhilaBelum ada peringkat
- JurnalDokumen12 halamanJurnalsheranadhilaBelum ada peringkat
- Depression in Temporal Lobe EpilepsyDokumen33 halamanDepression in Temporal Lobe EpilepsysheranadhilaBelum ada peringkat
- Unrecognized and Untreated FixDokumen7 halamanUnrecognized and Untreated FixsheranadhilaBelum ada peringkat
- Clinical Implication. Journal of Andrology, Vol. 24, No.6.: Daftar PustakaDokumen2 halamanClinical Implication. Journal of Andrology, Vol. 24, No.6.: Daftar PustakasheranadhilaBelum ada peringkat
- General Clinical Features:: DementiaDokumen10 halamanGeneral Clinical Features:: Dementiaanon_744017699Belum ada peringkat
- Depression in Temporal Lobe EpilepsyDokumen33 halamanDepression in Temporal Lobe EpilepsysheranadhilaBelum ada peringkat
- EpilepsiDokumen14 halamanEpilepsisheranadhilaBelum ada peringkat
- Meconium Aspiration SyndromeDokumen7 halamanMeconium Aspiration SyndromeAi Niech Inoel100% (1)
- 06 Disaster WardsDokumen15 halaman06 Disaster WardserwinBelum ada peringkat
- Penyimpanan InsulinDokumen5 halamanPenyimpanan InsulinAfina Laras SmaraneshaBelum ada peringkat
- Immature Ovarian TeratomaDokumen4 halamanImmature Ovarian TeratomaRocio SalazarBelum ada peringkat
- Health Problem Family Nursing Problem Goal of Care Objectives of Care Interventions Family-Nurse Contact Recources Required Criteria For EvaluationDokumen5 halamanHealth Problem Family Nursing Problem Goal of Care Objectives of Care Interventions Family-Nurse Contact Recources Required Criteria For EvaluationMadel AcobBelum ada peringkat
- Surgical, radiation, chemotherapy treatment options for gynecological cancersDokumen2 halamanSurgical, radiation, chemotherapy treatment options for gynecological cancersCarlos Del Carpio Enriquez100% (1)
- Mmaaj MenopauseDokumen3 halamanMmaaj MenopauseZarqa WaseemBelum ada peringkat
- PregnancyDokumen31 halamanPregnancyAnonymous Yqk1j9ABelum ada peringkat
- RCH program goals for reproductive health and child survivalDokumen2 halamanRCH program goals for reproductive health and child survivalAnnapurna DangetiBelum ada peringkat
- MM Ob Gyn Catalog WebDokumen100 halamanMM Ob Gyn Catalog Webthumper2madBelum ada peringkat
- Classification of Hernia: (CITATION Amr15 /L 1057)Dokumen3 halamanClassification of Hernia: (CITATION Amr15 /L 1057)dianBelum ada peringkat
- 3805594887Dokumen234 halaman3805594887gareththomasnzBelum ada peringkat
- Summer 2012: Ladybird Lake Lake Austin Lake Travis Lake Marble Falls Lake LBJ Lake BuchananDokumen64 halamanSummer 2012: Ladybird Lake Lake Austin Lake Travis Lake Marble Falls Lake LBJ Lake BuchananWaterways MagazineBelum ada peringkat
- Peptic Ulcer Disease (PUD) EditedDokumen9 halamanPeptic Ulcer Disease (PUD) EditedRashed ShatnawiBelum ada peringkat
- Population Welfare Program and ServicesDokumen57 halamanPopulation Welfare Program and Servicesadeel_khan_48Belum ada peringkat
- Antenatal Assessment of Foetal Wellbeing.Dokumen30 halamanAntenatal Assessment of Foetal Wellbeing.Kavya S MohanBelum ada peringkat
- The Gazette April 2013Dokumen12 halamanThe Gazette April 2013St George's Healthcare NHS TrustBelum ada peringkat
- Vol 4 DBR EPC AIIMS GKPR - 21.01.2018Dokumen234 halamanVol 4 DBR EPC AIIMS GKPR - 21.01.2018Shyam SinghBelum ada peringkat
- Psoriasis and Parapsoriasis Literature ReviewDokumen2 halamanPsoriasis and Parapsoriasis Literature ReviewBetharlitha PurLikaBelum ada peringkat
- Kel 3 A Midwifery Model of Care ForDokumen13 halamanKel 3 A Midwifery Model of Care ForWawa KurniaBelum ada peringkat
- Hospital Report PDFDokumen28 halamanHospital Report PDFGaurav Chaudhary Alig100% (1)
- Human Chorionic Gonadotropin (HCG) - HCG LevelsDokumen10 halamanHuman Chorionic Gonadotropin (HCG) - HCG Levelscristian andreiBelum ada peringkat
- Bryant 2018Dokumen11 halamanBryant 2018maritzabericesBelum ada peringkat
- Nelson MCQ PDFDokumen595 halamanNelson MCQ PDFPavan Kumar100% (5)
- Twin Pregnancy: Prenatal Issues - UpToDateDokumen70 halamanTwin Pregnancy: Prenatal Issues - UpToDateadityoBelum ada peringkat