Anda mungkin juga menyukai
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- VND ArticleDokumen11 halamanVND ArticleAmbar RahmanBelum ada peringkat
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- P ('t':'3', 'I':'668014889') D '' Var B Location Settimeout (Function ( If (Typeof Window - Iframe 'Undefined') ( B.href B.href ) ), 15000)Dokumen5 halamanP ('t':'3', 'I':'668014889') D '' Var B Location Settimeout (Function ( If (Typeof Window - Iframe 'Undefined') ( B.href B.href ) ), 15000)Ambar RahmanBelum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5795)
- NIH Public Access: Author ManuscriptDokumen12 halamanNIH Public Access: Author ManuscriptAmbar RahmanBelum ada peringkat
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- PatofisDokumen8 halamanPatofisAmbar RahmanBelum ada peringkat
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- 2012 2013 USFA Age Classification RestrictionsDokumen1 halaman2012 2013 USFA Age Classification RestrictionsAmbar RahmanBelum ada peringkat
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Chest PainDokumen30 halamanChest PainLamya ZamanBelum ada peringkat
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Pathway LeukemiaDokumen2 halamanPathway LeukemiaAmbar RahmanBelum ada peringkat
- How To Critically Appraise A PaperDokumen6 halamanHow To Critically Appraise A PaperAmbar RahmanBelum ada peringkat
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Sci9 q1 Mod1 Respiratory and Circulatory Systems Working With Other Organ Systems Version3Dokumen44 halamanSci9 q1 Mod1 Respiratory and Circulatory Systems Working With Other Organ Systems Version3Raniey MayolBelum ada peringkat
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Simpo 14 Sept 19Dokumen71 halamanSimpo 14 Sept 19Henry SBelum ada peringkat
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Ecg MCQSDokumen2 halamanEcg MCQSZafar Iqbal Manj100% (2)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- AcceptedDokumen28 halamanAcceptedChistian LassoBelum ada peringkat
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Angiography 170411210116Dokumen44 halamanAngiography 170411210116Ndikintum MaciasBelum ada peringkat
- NCP Decreased Cardiac OutputDokumen2 halamanNCP Decreased Cardiac OutputYamete KudasaiBelum ada peringkat
- Heart AnatomyDokumen7 halamanHeart AnatomyArjon BalaBelum ada peringkat
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- Vascular MCQ RoundsDokumen8 halamanVascular MCQ RoundsMohamed Elkhodary100% (1)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Pig Heart DissectionDokumen4 halamanPig Heart Dissectiongerardgil82Belum ada peringkat
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The Circulatory System (Heart)Dokumen3 halamanThe Circulatory System (Heart)NinaBelum ada peringkat
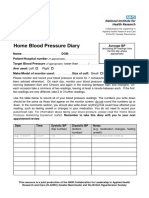
- Home Blood Pressure DiaryDokumen2 halamanHome Blood Pressure DiaryCherieBelum ada peringkat
- Entresto in Insuficienta CardiacaDokumen2 halamanEntresto in Insuficienta CardiacaRadu AndreiBelum ada peringkat
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- ECG UworldDokumen4 halamanECG UworldBaebee LouBelum ada peringkat
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1091)
- Start CPR Shout For Help/Activate Emergency Response: Give Oxygen Attach Monitor/DefibrillatorDokumen2 halamanStart CPR Shout For Help/Activate Emergency Response: Give Oxygen Attach Monitor/DefibrillatorFelicia ErikaBelum ada peringkat
- Antihypertensive Drugs.Dokumen35 halamanAntihypertensive Drugs.Abdul WahabBelum ada peringkat
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- BLS ExamDokumen5 halamanBLS ExamAhmed - Sawalha67% (6)
- Generic Name Brand Name Drug Class Mechanism of Action StructureDokumen4 halamanGeneric Name Brand Name Drug Class Mechanism of Action StructurenoelkiddoBelum ada peringkat
- Buerger's DiseaseDokumen41 halamanBuerger's DiseaseMay-ann CabreraBelum ada peringkat
- 30 Dec JoBs BY KHALIQ HASSAN - Watermarked PDFDokumen4 halaman30 Dec JoBs BY KHALIQ HASSAN - Watermarked PDFKamran Talpur100% (1)
- SDL DL BrochureDokumen2 halamanSDL DL BrochureNanda Nabilah UbayBelum ada peringkat
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- New York Heart Association (NYHA) Functional Classification in A Patient With Heart DiseaseDokumen2 halamanNew York Heart Association (NYHA) Functional Classification in A Patient With Heart Diseasemanikchopra111Belum ada peringkat
- Research Poster PresentationDokumen1 halamanResearch Poster Presentationapi-328441669Belum ada peringkat
- Masiag National High SchoolDokumen6 halamanMasiag National High SchoolJESSAN DE PEDROBelum ada peringkat
- Sir ClanDokumen109 halamanSir ClanJames AbendanBelum ada peringkat
- Anti-Arrhythmic Effect of Wild Honey AgainstDokumen10 halamanAnti-Arrhythmic Effect of Wild Honey AgainstMelivea Paez HerediaBelum ada peringkat
- A Case of Hypertension in Diabetes This Case Study Aims ToDokumen4 halamanA Case of Hypertension in Diabetes This Case Study Aims Towalit1101 mukrinin100% (1)
- Anesthetic Management For Woman With Single Ventricle Heart After BCPS Who Undergoes Curretage ProcedureDokumen3 halamanAnesthetic Management For Woman With Single Ventricle Heart After BCPS Who Undergoes Curretage ProcedureAnastasia AngelaBelum ada peringkat
- VastarelDokumen20 halamanVastarelKristen FieldsBelum ada peringkat
- Daftar InventarisDokumen47 halamanDaftar InventarisTri NastitiBelum ada peringkat
- 2.cardiac Output 17Dokumen38 halaman2.cardiac Output 17UmerBelum ada peringkat
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)