Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
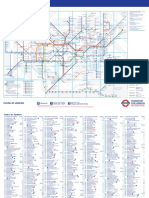
- Standard Tube MapDokumen2 halamanStandard Tube MapBenjamin Zari IIIBelum ada peringkat
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Hines Chaps 1 5 6 10 11Dokumen19 halamanHines Chaps 1 5 6 10 11dominscience1Belum ada peringkat
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Canterbury PDFDokumen1 halamanCanterbury PDFdominscience1Belum ada peringkat
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Cognitive PsychologyDokumen10 halamanCognitive Psychologydominscience1Belum ada peringkat
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Hansen, G - Deception in PSI ResearchDokumen57 halamanHansen, G - Deception in PSI Researchdominscience1Belum ada peringkat
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Moller, L - Pseudoscience or ProtoscienceDokumen3 halamanMoller, L - Pseudoscience or Protosciencedominscience1Belum ada peringkat
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Moller, L - Pseudoscience or ProtoscienceDokumen3 halamanMoller, L - Pseudoscience or Protosciencedominscience1Belum ada peringkat
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hansen, G - Deception in PSI ResearchDokumen57 halamanHansen, G - Deception in PSI Researchdominscience1Belum ada peringkat
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- DialoguesClinNeurosci 9 173Dokumen17 halamanDialoguesClinNeurosci 9 173dominscience1Belum ada peringkat
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- Cognitive PsychologyDokumen10 halamanCognitive Psychologydominscience1Belum ada peringkat
- Reader, C - Khufu Knew The SphinxDokumen19 halamanReader, C - Khufu Knew The Sphinxdominscience1Belum ada peringkat
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Cognitive PsychologyDokumen10 halamanCognitive Psychologydominscience1Belum ada peringkat
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- Spirit Slate Writing and Kindred PhenomenaDokumen89 halamanSpirit Slate Writing and Kindred Phenomenadominscience1Belum ada peringkat
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Playing Ground PartIDokumen3 halamanThe Playing Ground PartIdominscience1Belum ada peringkat
- Did A Five-Day Camp Without Digital Devices Really Boost Children's Interpersonal Skills?Dokumen2 halamanDid A Five-Day Camp Without Digital Devices Really Boost Children's Interpersonal Skills?dominscience1Belum ada peringkat
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Breaking ResearchDokumen2 halamanBreaking Researchdominscience1Belum ada peringkat
- Using "Programmable" Antibiotics To Attack Drug-Resistant MicrobesDokumen3 halamanUsing "Programmable" Antibiotics To Attack Drug-Resistant Microbesdominscience1Belum ada peringkat
- The Playing Ground PartDokumen3 halamanThe Playing Ground Partdominscience1Belum ada peringkat
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Tricksy Insects Sing A Song of Love andDokumen2 halamanTricksy Insects Sing A Song of Love anddominscience1Belum ada peringkat
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Neurobiological Basis of A HumanDokumen3 halamanThe Neurobiological Basis of A Humandominscience1Belum ada peringkat
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Sleeping Brains Understand WordsDokumen2 halamanSleeping Brains Understand Wordsdominscience1Belum ada peringkat
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- The GutDokumen2 halamanThe Gutdominscience1Belum ada peringkat
- 2007 PN Test PreparationDokumen29 halaman2007 PN Test Preparationfairwoods80% (5)
- Inhibitory Activity and Phytochemical Assessment of Ethno-Medicinal Plants Against Some Human Pathogenic BacteriaDokumen8 halamanInhibitory Activity and Phytochemical Assessment of Ethno-Medicinal Plants Against Some Human Pathogenic BacteriaLavanya Priya SathyanBelum ada peringkat
- Classical Conditioning Practice - Print - QuizizzDokumen3 halamanClassical Conditioning Practice - Print - Quizizzsafa g100% (1)
- Restless Leg Syndrome: The Most Common Disorder You Have Never Heard Of."Dokumen20 halamanRestless Leg Syndrome: The Most Common Disorder You Have Never Heard Of."Maulida Manurung100% (1)
- African Drumming As A Medium To Promote EmotionalDokumen345 halamanAfrican Drumming As A Medium To Promote EmotionalRodrigo ZúñigaBelum ada peringkat
- Turning ABGs Into Childs PlayDokumen35 halamanTurning ABGs Into Childs PlayLucyz KlosetBelum ada peringkat
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Effects of A Cognitive-Behavioral Intervention On Career IndecisionDokumen14 halamanEffects of A Cognitive-Behavioral Intervention On Career IndecisionJuLievee LentejasBelum ada peringkat
- Dynamic Psychoth For Personality DisordDokumen285 halamanDynamic Psychoth For Personality DisordPetzyMarian100% (1)
- Birth of CosmopathyDokumen7 halamanBirth of CosmopathyKirti BetaiBelum ada peringkat
- Theoretical Application of Kohutian Theory To Anorexia and Bulimia NervosaDokumen12 halamanTheoretical Application of Kohutian Theory To Anorexia and Bulimia NervosakelkarinBelum ada peringkat
- Noor PDFDokumen826 halamanNoor PDFAnonymous d1CGjMTi100% (1)
- Obsessive Compulsive Disorder Punjabi Instant Download 1Dokumen3 halamanObsessive Compulsive Disorder Punjabi Instant Download 1Ameera ChauhanBelum ada peringkat
- Family Therapy CorrectedDokumen8 halamanFamily Therapy Correctedalolika dolaiBelum ada peringkat
- 2017 11th Annual Women's Hot Yoga Retreat TimelineDokumen4 halaman2017 11th Annual Women's Hot Yoga Retreat TimelineBikram Retreat100% (1)
- Seminars in Oncology: Male Breast Cancer: Epidemiology and Risk FactorsDokumen6 halamanSeminars in Oncology: Male Breast Cancer: Epidemiology and Risk FactorsGina Kristina NanginBelum ada peringkat
- Chronic Constipation: Guest Editor: Bhim S. PandhiDokumen5 halamanChronic Constipation: Guest Editor: Bhim S. PandhiAndreea PopescuBelum ada peringkat
- Case Study Uterine MyomaDokumen30 halamanCase Study Uterine MyomaNikko Dela Cruz100% (1)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Development of A Classification System For Periodontal Diseases and Conditions - Armitage 1999Dokumen6 halamanDevelopment of A Classification System For Periodontal Diseases and Conditions - Armitage 1999csryderBelum ada peringkat
- Dosage CalculationsDokumen39 halamanDosage Calculationssalak9462900% (1)
- Depo FoamDokumen12 halamanDepo FoamFilip IlievskiBelum ada peringkat
- Or JournalDokumen4 halamanOr JournalKim_Bayani_6017Belum ada peringkat
- Assignment: Carl RogersDokumen5 halamanAssignment: Carl RogersSheshwarya PBelum ada peringkat
- The Handout On PEH Lev II - 7 July 2013 PDFDokumen85 halamanThe Handout On PEH Lev II - 7 July 2013 PDFAnonymous X6VPZL5nAe100% (2)
- Gout ArthritisDokumen8 halamanGout ArthritisMarie Nelle Escriba LimpocoBelum ada peringkat
- Aspergillus and Vaginal Colonization-2329-8731.1000e115Dokumen2 halamanAspergillus and Vaginal Colonization-2329-8731.1000e115Hervis Francisco FantiniBelum ada peringkat
- TrombocitopeniaDokumen10 halamanTrombocitopeniabyrock66Belum ada peringkat
- EMDR Art TherapyDokumen6 halamanEMDR Art TherapyStayOccupiedBelum ada peringkat
- Penyaji: Ayu Iswandari Raharjo Pembimbing 1:Dr. Dr. M. Zafrullah Arifin, SP - Bs (K) Dr. Ahmad Faried, SP - Bs (K) PHDDokumen14 halamanPenyaji: Ayu Iswandari Raharjo Pembimbing 1:Dr. Dr. M. Zafrullah Arifin, SP - Bs (K) Dr. Ahmad Faried, SP - Bs (K) PHDayuBelum ada peringkat
- WWW Healingqigong Org 8 Section BrocadeDokumen8 halamanWWW Healingqigong Org 8 Section BrocadeqpidoneuroBelum ada peringkat
- Approaches of CunsellingDokumen5 halamanApproaches of CunsellingNelson Grande CalimagBelum ada peringkat
- The Obesity Code: Unlocking the Secrets of Weight LossDari EverandThe Obesity Code: Unlocking the Secrets of Weight LossPenilaian: 4 dari 5 bintang4/5 (6)
- The Age of Magical Overthinking: Notes on Modern IrrationalityDari EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityPenilaian: 4 dari 5 bintang4/5 (28)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsDari EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsBelum ada peringkat