Anda mungkin juga menyukai
- Identifying Child Abuse Fatalities During Infancy: Clinical ReportDokumen11 halamanIdentifying Child Abuse Fatalities During Infancy: Clinical ReportJesse M. MassieBelum ada peringkat
- Oral and Dental Aspects of Child Abuse and Neglect: Clinical ReportDokumen10 halamanOral and Dental Aspects of Child Abuse and Neglect: Clinical ReportJesse M. MassieBelum ada peringkat
- Effective Discipline To Raise Healthy Children: Policy StatementDokumen12 halamanEffective Discipline To Raise Healthy Children: Policy StatementJesse M. MassieBelum ada peringkat
- Jpeds Aom 208Dokumen3 halamanJpeds Aom 208Jesse M. MassieBelum ada peringkat
- i-PASS OBSERVATION TOOLDokumen1 halamani-PASS OBSERVATION TOOLJesse M. MassieBelum ada peringkat
- Ongoing Pediatric Health Care For The Child Who Has Been MaltreatedDokumen18 halamanOngoing Pediatric Health Care For The Child Who Has Been MaltreatedJesse M. MassieBelum ada peringkat
- IJMEDokumen7 halamanIJMEJesse M. MassieBelum ada peringkat
- What Is Child Abuse and Neglect? Recognizing The Signs and SymptomsDokumen8 halamanWhat Is Child Abuse and Neglect? Recognizing The Signs and SymptomsJesse M. MassieBelum ada peringkat
- Making The Most of Mentors: A Guide For MenteesDokumen5 halamanMaking The Most of Mentors: A Guide For MenteesJesse M. MassieBelum ada peringkat
- Cbig Cross-ReportingDokumen25 halamanCbig Cross-ReportingJesse M. MassieBelum ada peringkat
- Preventing Adverse Childhood Experiences (Aces) :: Leveraging The Best Available EvidenceDokumen40 halamanPreventing Adverse Childhood Experiences (Aces) :: Leveraging The Best Available EvidenceJesse M. MassieBelum ada peringkat
- dBA PROTECT YOUR HEARINGDokumen4 halamandBA PROTECT YOUR HEARINGJesse M. MassieBelum ada peringkat
- Suidi Oklahoma ProviderDokumen28 halamanSuidi Oklahoma ProviderJesse M. MassieBelum ada peringkat
- Status EpileticusDokumen2 halamanStatus EpileticusJesse M. MassieBelum ada peringkat
- Male Victims of Intimate Partner Violence: Did You Know?Dokumen3 halamanMale Victims of Intimate Partner Violence: Did You Know?Jesse M. MassieBelum ada peringkat
- Noisey PlanetDokumen1 halamanNoisey PlanetJesse M. MassieBelum ada peringkat
- Minority YouthDokumen28 halamanMinority YouthJesse M. MassieBelum ada peringkat
- COVID Positive/PUI: PAPR Prioritization MatrixDokumen1 halamanCOVID Positive/PUI: PAPR Prioritization MatrixJesse M. MassieBelum ada peringkat
- Kinshipguardianship PDFDokumen139 halamanKinshipguardianship PDFJesse M. MassieBelum ada peringkat
- Intimate Partner Violence, Sexual Violence, Stalking: Before The Age of 18Dokumen1 halamanIntimate Partner Violence, Sexual Violence, Stalking: Before The Age of 18Jesse M. MassieBelum ada peringkat
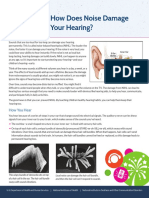
- How Does Noise Damage Your Hearing?Dokumen2 halamanHow Does Noise Damage Your Hearing?Jesse M. MassieBelum ada peringkat
- Domestic Violence Oklahoma 2017Dokumen44 halamanDomestic Violence Oklahoma 2017Jesse M. MassieBelum ada peringkat
- CDC Capacity BuildingDokumen16 halamanCDC Capacity BuildingJesse M. MassieBelum ada peringkat
- How Loud Is Too LoudDokumen2 halamanHow Loud Is Too LoudJesse M. MassieBelum ada peringkat
- Aap Food Insecurity Toolkit For ProvidersDokumen39 halamanAap Food Insecurity Toolkit For ProvidersJesse M. MassieBelum ada peringkat
- In Drinking Water: Sources of LEADDokumen1 halamanIn Drinking Water: Sources of LEADJesse M. MassieBelum ada peringkat
- Advancing Health Equity: A Practitioner'S Guide ForDokumen132 halamanAdvancing Health Equity: A Practitioner'S Guide ForJesse M. MassieBelum ada peringkat
- Fireworks ShowDokumen2 halamanFireworks ShowJesse M. MassieBelum ada peringkat
- Cbig Child Abuse and Neglect Fatalities 2017Dokumen8 halamanCbig Child Abuse and Neglect Fatalities 2017Jesse M. MassieBelum ada peringkat
- Essentials For Childhood:: Steps To Create Safe, Stable, Nurturing Relationships and EnvironmentsDokumen1 halamanEssentials For Childhood:: Steps To Create Safe, Stable, Nurturing Relationships and EnvironmentsJesse M. MassieBelum ada peringkat
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- List of 2 Years AffiliationDokumen15 halamanList of 2 Years AffiliationAahad AmeenBelum ada peringkat
- CV of DoctorDokumen1 halamanCV of DoctorBobby Jatt0% (1)
- HEALTHDokumen28 halamanHEALTHKristine SaulerBelum ada peringkat
- NYS Office of Professional Conduct Opens Investigation of Controversial Psychiatrist Kelly Brogan (11/24/20) + My Complaint Re: Her License (3/22/20)Dokumen5 halamanNYS Office of Professional Conduct Opens Investigation of Controversial Psychiatrist Kelly Brogan (11/24/20) + My Complaint Re: Her License (3/22/20)Peter M. Heimlich100% (1)
- HIS-district LaboratoryDokumen6 halamanHIS-district LaboratoryEricka GenoveBelum ada peringkat
- BSN Curriculum 20 21 English 1Dokumen3 halamanBSN Curriculum 20 21 English 1ROSE DIVINAGRACIABelum ada peringkat
- Resume PDFDokumen1 halamanResume PDFapi-353271874Belum ada peringkat
- James Sloan Takes Firm Stand On Issues Important To Tennessee House of Representatives District 63Dokumen4 halamanJames Sloan Takes Firm Stand On Issues Important To Tennessee House of Representatives District 63PR.comBelum ada peringkat
- Experts Validation TableDokumen20 halamanExperts Validation TableDeepti KukretiBelum ada peringkat
- Continuing Competency Log PrintDokumen2 halamanContinuing Competency Log PrintBobBelum ada peringkat
- Clinical Applications of Nursing DiagnosisDokumen768 halamanClinical Applications of Nursing DiagnosisAyaz Ahmed Brohi100% (1)
- 6450a6d07795498d Derma360reportDokumen12 halaman6450a6d07795498d Derma360reportNeelam PahujaBelum ada peringkat
- Medical - Strips (Medical Grade vs. "Hospital Grade")Dokumen22 halamanMedical - Strips (Medical Grade vs. "Hospital Grade")Nirav DesaiBelum ada peringkat
- Pharma DirectoryDokumen1.899 halamanPharma DirectoryVandana Tyagi100% (2)
- Changes in Hospital Competitive StrategyDokumen23 halamanChanges in Hospital Competitive Strategyanantomi100% (1)
- Panic Disorder: GuidelineDokumen3 halamanPanic Disorder: Guidelineputri weniBelum ada peringkat
- (Medical Radiology) Lluís Donoso-Bach, Giles W. L. Boland - Quality and Safety in Imaging-Springer International Publishing (2018)Dokumen187 halaman(Medical Radiology) Lluís Donoso-Bach, Giles W. L. Boland - Quality and Safety in Imaging-Springer International Publishing (2018)Piotr JankowskiBelum ada peringkat
- Project Seminar Hospice FedoraDokumen3 halamanProject Seminar Hospice FedoralalithaBelum ada peringkat
- ��تجميعات الفارما�Dokumen4 halaman��تجميعات الفارما�Turky TurkyBelum ada peringkat
- You Are Dangerous To Your Health CRAWFORDDokumen18 halamanYou Are Dangerous To Your Health CRAWFORDGonzalo PaezBelum ada peringkat
- Pola Penggunaan Obat Antihipertensi Pada Pasien Hipertensi: Teti Sutriati Tuloli, Nur Rasdianah, Faradilasandi TahalaDokumen9 halamanPola Penggunaan Obat Antihipertensi Pada Pasien Hipertensi: Teti Sutriati Tuloli, Nur Rasdianah, Faradilasandi TahalaSifa ShopingBelum ada peringkat
- Healthcare & Life Sciences ReviewDokumen47 halamanHealthcare & Life Sciences Reviewmercadia59970% (1)
- Food Handler Training CoursesDokumen2 halamanFood Handler Training CoursesSai Ram ChanduriBelum ada peringkat
- Cv. Dr. Saldy YusufDokumen6 halamanCv. Dr. Saldy YusufMuhammad FaturrahmanBelum ada peringkat
- Physical Education and Health 12Dokumen2 halamanPhysical Education and Health 12Jenia Alexis CapaBelum ada peringkat
- Dental Claim FormDokumen2 halamanDental Claim Formmiranda criggerBelum ada peringkat
- Francois Gremy (Autosaved)Dokumen7 halamanFrancois Gremy (Autosaved)Donya GholamiBelum ada peringkat
- Dental Officer Information - e (1989)Dokumen10 halamanDental Officer Information - e (1989)Marian GarciaBelum ada peringkat
- Policies Under NMHC Act 2017Dokumen2 halamanPolicies Under NMHC Act 2017SAKSHI SHRIPAL SHAH 1833474Belum ada peringkat
- James Belgira Tamayo, RMT, MD James Belgira Tamayo, RMT, MDDokumen1 halamanJames Belgira Tamayo, RMT, MD James Belgira Tamayo, RMT, MDfilchibuffBelum ada peringkat