Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Chronic Renal Failure Long CaseDokumen2 halamanChronic Renal Failure Long CaseUsman Ali AkbarBelum ada peringkat
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Chronic Renal Failure: Concise Long Case ApproachDokumen3 halamanChronic Renal Failure: Concise Long Case ApproachUsman Ali AkbarBelum ada peringkat
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Renal Tubular Acidosis SummaryDokumen1 halamanRenal Tubular Acidosis SummaryUsman Ali AkbarBelum ada peringkat
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (894)
- CRF Wtih Fluid Overload MX Pathway - AdjDokumen1 halamanCRF Wtih Fluid Overload MX Pathway - AdjUsman Ali AkbarBelum ada peringkat
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Urinary Tract Infection & PyelonephritisDokumen3 halamanUrinary Tract Infection & PyelonephritisUsman Ali AkbarBelum ada peringkat
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- GI Bleeding Team Work - 2nd EditionDokumen9 halamanGI Bleeding Team Work - 2nd EditionUsman Ali AkbarBelum ada peringkat
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Nephrotic SyndromeDokumen2 halamanNephrotic SyndromeUsman Ali AkbarBelum ada peringkat
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- CRF Wtih Fluid Overload MX PathwayDokumen1 halamanCRF Wtih Fluid Overload MX PathwayUsman Ali AkbarBelum ada peringkat
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Polycystic Kidneys: Adult PKD: ComplicationsDokumen1 halamanPolycystic Kidneys: Adult PKD: ComplicationsUsman Ali AkbarBelum ada peringkat
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- Renal Tubular Acidosis Summary - AdjDokumen1 halamanRenal Tubular Acidosis Summary - AdjUsman Ali AkbarBelum ada peringkat
- Dialysis Treatment Options: Peritoneal Dialysis vs HemodialysisDokumen2 halamanDialysis Treatment Options: Peritoneal Dialysis vs HemodialysisUsman Ali AkbarBelum ada peringkat
- Renal TransplantDokumen2 halamanRenal TransplantUsman Ali AkbarBelum ada peringkat
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- GI Bleeding Team Work - 2nd EditionDokumen9 halamanGI Bleeding Team Work - 2nd EditionUsman Ali AkbarBelum ada peringkat
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- Obstructive Airway Diseases ExplainedDokumen53 halamanObstructive Airway Diseases ExplainedUsman Ali AkbarBelum ada peringkat
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Ibs Presentation PDFDokumen18 halamanIbs Presentation PDFUsman Ali AkbarBelum ada peringkat
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
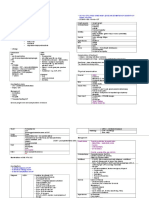
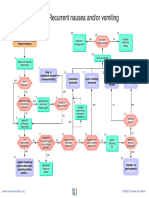
- Recurrent Nausea Andor VomitingDokumen8 halamanRecurrent Nausea Andor VomitingUsman Ali AkbarBelum ada peringkat
- Anaemia in PregnancyDokumen13 halamanAnaemia in PregnancyUsman Ali AkbarBelum ada peringkat
- King Khalid University Hospital Department of Obstetrics & Gyncology Course 481Dokumen40 halamanKing Khalid University Hospital Department of Obstetrics & Gyncology Course 481Usman Ali AkbarBelum ada peringkat
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Anaemia in PregnancyDokumen13 halamanAnaemia in PregnancyUsman Ali AkbarBelum ada peringkat
- IBS Pathophysiology & ManagementDokumen18 halamanIBS Pathophysiology & ManagementUsman Ali AkbarBelum ada peringkat
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- CORD PROLAPSE GUIDEDokumen2 halamanCORD PROLAPSE GUIDEUsman Ali AkbarBelum ada peringkat
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- Clinical Calendar 2016-2018Dokumen3 halamanClinical Calendar 2016-2018NickBelum ada peringkat
- GRAM NEGATIVE RODS (5) Fastidious Organisms From Animal Sources (A)Dokumen1 halamanGRAM NEGATIVE RODS (5) Fastidious Organisms From Animal Sources (A)Usman Ali AkbarBelum ada peringkat
- Recurrent VomitingDokumen16 halamanRecurrent VomitingUsman Ali AkbarBelum ada peringkat
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Subject: Permission For Badminton Court NID, Multan: TH THDokumen1 halamanSubject: Permission For Badminton Court NID, Multan: TH THUsman Ali AkbarBelum ada peringkat
- When Hope DiesDokumen2 halamanWhen Hope DiesUsman Ali AkbarBelum ada peringkat
- Organophosphate Poisoning Signs, Symptoms, and TreatmentDokumen23 halamanOrganophosphate Poisoning Signs, Symptoms, and TreatmentUsman Ali AkbarBelum ada peringkat
- Foreign Visiting Student Medical Status Form PDFDokumen1 halamanForeign Visiting Student Medical Status Form PDFUsman Ali AkbarBelum ada peringkat
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- TSMEntry 2Dokumen1 halamanTSMEntry 2Usman Ali AkbarBelum ada peringkat
- Diseases of The StomachDokumen17 halamanDiseases of The StomachUsman Ali AkbarBelum ada peringkat
- Curs DR PellegrinoDokumen1 halamanCurs DR PellegrinorfandreiBelum ada peringkat
- Ethical Counselling and Medical Decision-Making in The Era of Personalised Medicine A Practice-Oriented Guide PDFDokumen129 halamanEthical Counselling and Medical Decision-Making in The Era of Personalised Medicine A Practice-Oriented Guide PDFEddyYuristoBelum ada peringkat
- Case StudyDokumen6 halamanCase StudyMattBelum ada peringkat
- Dolan 1996Dokumen7 halamanDolan 1996Ainia TaufiqaBelum ada peringkat
- Daftar Pustaka AsihDokumen5 halamanDaftar Pustaka AsihKhansaBelum ada peringkat
- Piezosurgery: By, Prathusha.U CRI Department of Public Health Dentistry Chettinad Dental CollegeDokumen36 halamanPiezosurgery: By, Prathusha.U CRI Department of Public Health Dentistry Chettinad Dental CollegePrathusha Umakhanth100% (1)
- Drug StudyDokumen17 halamanDrug StudyTherese ArellanoBelum ada peringkat
- Najib Khalife - Advances in TPET and Its Immunomodulatory Effect in NMDDokumen6 halamanNajib Khalife - Advances in TPET and Its Immunomodulatory Effect in NMDMarina ShinkoBelum ada peringkat
- Dialog Convincing, Consoling, Persuading, Encouraging, Apologizing, Disclaiming, RequestingDokumen4 halamanDialog Convincing, Consoling, Persuading, Encouraging, Apologizing, Disclaiming, RequestingmeliaBelum ada peringkat
- EN Quick Reference Guide Fabian HFOi-V4.0Dokumen30 halamanEN Quick Reference Guide Fabian HFOi-V4.0Tanzimul IslamBelum ada peringkat
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- N120 Final Review PDFDokumen7 halamanN120 Final Review PDFsutopianoBelum ada peringkat
- Guía OxigenoterapiaDokumen39 halamanGuía OxigenoterapiaSMIBA MedicinaBelum ada peringkat
- Insights Into Veterinary Endocrinology - Diagnostic Approach To PU - PD - Urine Specific GravityDokumen4 halamanInsights Into Veterinary Endocrinology - Diagnostic Approach To PU - PD - Urine Specific GravityHusnat hussainBelum ada peringkat
- Coliform BacteriaDokumen4 halamanColiform BacteriaLalu Novan SatriaBelum ada peringkat
- Led Astray: Clinical Problem-SolvingDokumen6 halamanLed Astray: Clinical Problem-SolvingmeganBelum ada peringkat
- Methods For The Euthanasia of Dogs and Cats - EnglishDokumen28 halamanMethods For The Euthanasia of Dogs and Cats - Englishapi-266985430Belum ada peringkat
- Last health purchase, service used and who shared informationDokumen17 halamanLast health purchase, service used and who shared informationRiccalhynne MagpayoBelum ada peringkat
- D.O School InformationDokumen102 halamanD.O School Informationkape1oneBelum ada peringkat
- Seth AnswerDokumen27 halamanSeth AnswerDave BiscobingBelum ada peringkat
- Objective Structured Clinical Examination (Osce) : Examinee'S Perception at Department of Pediatrics and Child Health, Jimma UniversityDokumen6 halamanObjective Structured Clinical Examination (Osce) : Examinee'S Perception at Department of Pediatrics and Child Health, Jimma UniversityNuurBelum ada peringkat
- Effects of Healthcare Environmental Design On Medical Outcomes PDFDokumen11 halamanEffects of Healthcare Environmental Design On Medical Outcomes PDFAgnes Cheverloo Castillo100% (1)
- OutputDokumen1 halamanOutputmsenthamizharasaBelum ada peringkat
- Care for a Client with LeptospirosisDokumen4 halamanCare for a Client with LeptospirosisLyndon SayongBelum ada peringkat
- Evidence Based Practice in Nursing BinuDokumen51 halamanEvidence Based Practice in Nursing BinuBinu Joshva100% (2)
- Hyperglycemia in Critically Ill Management (: From ICU To The Ward)Dokumen20 halamanHyperglycemia in Critically Ill Management (: From ICU To The Ward)destiana samputriBelum ada peringkat
- Drugs Acting On The Gastrointestinal System PDFDokumen18 halamanDrugs Acting On The Gastrointestinal System PDFMarc De JesusBelum ada peringkat
- Business Plan Analysis - 08 1: SFHN/SJ&G Oxalepsy (Oxcarbazipine300 & 600 MG)Dokumen63 halamanBusiness Plan Analysis - 08 1: SFHN/SJ&G Oxalepsy (Oxcarbazipine300 & 600 MG)Muhammad SalmanBelum ada peringkat
- Research EssayDokumen12 halamanResearch Essayapi-608972617Belum ada peringkat
- Repositioning an Inverted UterusDokumen5 halamanRepositioning an Inverted Uterusshraddha vermaBelum ada peringkat
- New Technologies Related To Public Health Electronic InformationDokumen22 halamanNew Technologies Related To Public Health Electronic InformationKhams TolentinoBelum ada peringkat
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionDari EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionPenilaian: 4 dari 5 bintang4/5 (402)
- Why We Die: The New Science of Aging and the Quest for ImmortalityDari EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityPenilaian: 3.5 dari 5 bintang3.5/5 (2)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisDari EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisPenilaian: 4 dari 5 bintang4/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedDari EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedPenilaian: 5 dari 5 bintang5/5 (78)
- The Age of Magical Overthinking: Notes on Modern IrrationalityDari EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityPenilaian: 4 dari 5 bintang4/5 (13)