Anda mungkin juga menyukai
- Multifocal Osteoarticular Tuberculosis in Children: Journal of Orthopaedic Surgery 2011 19 (3) :336-40Dokumen5 halamanMultifocal Osteoarticular Tuberculosis in Children: Journal of Orthopaedic Surgery 2011 19 (3) :336-40Suci IryandaBelum ada peringkat
- A Case Report On Potts Spine Spinal TubeDokumen3 halamanA Case Report On Potts Spine Spinal TubeyaneemayBelum ada peringkat
- Practice: Kikuchi-Fujimoto Disease: Lymphadenopathy in SiblingsDokumen4 halamanPractice: Kikuchi-Fujimoto Disease: Lymphadenopathy in SiblingsBobby Faisyal RakhmanBelum ada peringkat
- Acute Hypotonia in An Infant (2017)Dokumen3 halamanAcute Hypotonia in An Infant (2017)nikos.alexandrBelum ada peringkat
- Pe 07070Dokumen4 halamanPe 07070Mich KingsBelum ada peringkat
- Case Report: Vertigo As A Predominant Manifestation of NeurosarcoidosisDokumen5 halamanCase Report: Vertigo As A Predominant Manifestation of NeurosarcoidosisDjumadi AkbarBelum ada peringkat
- ALS1Dokumen4 halamanALS1Jhoana Rose Joaquin SantosBelum ada peringkat
- Admin A 10 1 85 3b9f306Dokumen8 halamanAdmin A 10 1 85 3b9f306Dyanne BautistaBelum ada peringkat
- Ovadia 2007Dokumen7 halamanOvadia 2007uditBelum ada peringkat
- P ('t':'3', 'I':'3054463181') D '' Var B Location Settimeout (Function ( If (Typeof Window - Iframe 'Undefined') ( B.href B.href ) ), 15000)Dokumen9 halamanP ('t':'3', 'I':'3054463181') D '' Var B Location Settimeout (Function ( If (Typeof Window - Iframe 'Undefined') ( B.href B.href ) ), 15000)Meis MalirmaseleBelum ada peringkat
- Founier GangrenDokumen5 halamanFounier GangrenJohannes MarpaungBelum ada peringkat
- Immunoglobulin A (Iga) NephropathyDokumen25 halamanImmunoglobulin A (Iga) NephropathyErika Joy ImperioBelum ada peringkat
- A Clinical Epidemiological Study in 2169 Patients With VertigoDokumen6 halamanA Clinical Epidemiological Study in 2169 Patients With VertigoDinar Yuniswandari KnightleyBelum ada peringkat
- 631-Article Text-2378-1-10-20180830Dokumen6 halaman631-Article Text-2378-1-10-20180830azizhamoudBelum ada peringkat
- Efficacy of Epley's Maneuver in Treating BPPV Patients: A Prospective Observational StudyDokumen8 halamanEfficacy of Epley's Maneuver in Treating BPPV Patients: A Prospective Observational StudyAgnestya RauleBelum ada peringkat
- Causes of Death in Multiple System AtrophyDokumen3 halamanCauses of Death in Multiple System Atrophybenghoe77Belum ada peringkat
- Osteogenesisimperfecta in The Newborn: About A CaseDokumen3 halamanOsteogenesisimperfecta in The Newborn: About A CaseIJAR JOURNALBelum ada peringkat
- Neck Swelling: Unusual Manifestation of Pott's Spine: Egyptian Journal of Ear, Nose, Throat and Allied SciencesDokumen3 halamanNeck Swelling: Unusual Manifestation of Pott's Spine: Egyptian Journal of Ear, Nose, Throat and Allied SciencesSonia RogersBelum ada peringkat
- tmp2CD0 TMPDokumen4 halamantmp2CD0 TMPFrontiersBelum ada peringkat
- Potter'S Syndrome: A Study of 15 Patients: Original ArticleDokumen4 halamanPotter'S Syndrome: A Study of 15 Patients: Original ArticleyanuarizkaBelum ada peringkat
- The Use of Traditional Chinese Veterinary Medicine in The Treatment of 5 Cases of Neoplastic Bone DiseaseDokumen12 halamanThe Use of Traditional Chinese Veterinary Medicine in The Treatment of 5 Cases of Neoplastic Bone DiseaseDonnaBelum ada peringkat
- Laringomalacia - Nursing CareDokumen9 halamanLaringomalacia - Nursing CareRirin Muthia ZukhraBelum ada peringkat
- Ijced 3 (3) 101-109Dokumen9 halamanIjced 3 (3) 101-109GembongSatriaMahardhikaBelum ada peringkat
- Skeletal Manifestations of Scurvy - Case Report DubaiDokumen5 halamanSkeletal Manifestations of Scurvy - Case Report DubaigistaluvikaBelum ada peringkat
- Clinical Feature and Etiology of Septic Arthritis and Osteomyelitis in ChildrenDokumen5 halamanClinical Feature and Etiology of Septic Arthritis and Osteomyelitis in ChildrenIfit Bagus ApriantonoBelum ada peringkat
- Failure To ThriveDokumen3 halamanFailure To ThrivefernandoBelum ada peringkat
- Reacciones Posturales de VojtaDokumen5 halamanReacciones Posturales de VojtaHéctor MartínezBelum ada peringkat
- Oral Care Reduces Pneumonia in Older Patients in Nursing HomesDokumen4 halamanOral Care Reduces Pneumonia in Older Patients in Nursing HomesYasir MahfudBelum ada peringkat
- Mistaken Identity Reporting Two Cases of Rare Fo 2024 International JournalDokumen7 halamanMistaken Identity Reporting Two Cases of Rare Fo 2024 International JournalRonald QuezadaBelum ada peringkat
- The NORSE (New-Onset Refractory Status Epileptic Us) SyndromeDokumen4 halamanThe NORSE (New-Onset Refractory Status Epileptic Us) Syndromebenghooi75Belum ada peringkat
- Disease Characteristics of Filipino Ankylosing Spondylitis Patients in Metro Manila Rheumatology ClinicsDokumen5 halamanDisease Characteristics of Filipino Ankylosing Spondylitis Patients in Metro Manila Rheumatology ClinicsaxxoBelum ada peringkat
- Epidemiology of Pediatric Acute Encephalitis/Encephalopathy in JapanDokumen7 halamanEpidemiology of Pediatric Acute Encephalitis/Encephalopathy in Japaneko andryBelum ada peringkat
- Animal Models 1Dokumen4 halamanAnimal Models 1Sanem CimenBelum ada peringkat
- Case Study AGN MINEDokumen66 halamanCase Study AGN MINEkappaBelum ada peringkat
- Medicine: Systemic Lupus Erythematosus With Guillian - Barre SyndromeDokumen5 halamanMedicine: Systemic Lupus Erythematosus With Guillian - Barre SyndromeShri RamBelum ada peringkat
- Colorectal CancerDokumen50 halamanColorectal CancerHans Chester Rirao Capinding100% (2)
- WhateverDokumen3 halamanWhatevergaurav sharmaBelum ada peringkat
- Tetanus: Clostridium Tetani. The Disease Was First Described in The 14th Century by John of ArderneDokumen5 halamanTetanus: Clostridium Tetani. The Disease Was First Described in The 14th Century by John of Ardernedefitri sariningtyasBelum ada peringkat
- Lazy Leucocyte SyndromeDokumen2 halamanLazy Leucocyte SyndromeDragos BourosBelum ada peringkat
- Spectrum of Congenital Malformations in Newborns: in A Medical College Hospital in South IndiaDokumen4 halamanSpectrum of Congenital Malformations in Newborns: in A Medical College Hospital in South Indianikhil00007Belum ada peringkat
- Guide to Pediatric Urology and Surgery in Clinical PracticeDari EverandGuide to Pediatric Urology and Surgery in Clinical PracticeBelum ada peringkat
- Clinical Cases in Pediatric Peripheral NeuropathyDokumen23 halamanClinical Cases in Pediatric Peripheral NeuropathyMateen ShukriBelum ada peringkat
- Spinal Tuberculosis Potts DiseaseDokumen3 halamanSpinal Tuberculosis Potts Diseaseshrishti shadangiBelum ada peringkat
- Sindrom PatauDokumen12 halamanSindrom PatauIoana PaulaBelum ada peringkat
- Prevalence and Risk Factors of Lumbar Spondylolisthesis in Elderly Chinese Men and WomenDokumen8 halamanPrevalence and Risk Factors of Lumbar Spondylolisthesis in Elderly Chinese Men and Womenrobert silitongaBelum ada peringkat
- 2479 ArticleDokumen5 halaman2479 Articleclbenitez52Belum ada peringkat
- Predictors of Unprovoked Seizure After Febrile Seizure: Short-Term OutcomesDokumen7 halamanPredictors of Unprovoked Seizure After Febrile Seizure: Short-Term Outcomesrizad mohamadBelum ada peringkat
- Hirschsprung Disease: Historical NotesDokumen17 halamanHirschsprung Disease: Historical Notesdesthalia cyatraningtyasBelum ada peringkat
- Advance Publication by J-STAGE: Japanese Journal of Infectious DiseasesDokumen8 halamanAdvance Publication by J-STAGE: Japanese Journal of Infectious DiseasesEdgar Azael GarciaBelum ada peringkat
- Urosepsis Is The Most Common Complication of Purn-Belly SyndromeDokumen4 halamanUrosepsis Is The Most Common Complication of Purn-Belly Syndromeraisa desti ardiantyBelum ada peringkat
- Case+Study AGN MINEDokumen66 halamanCase+Study AGN MINEJm BernardoBelum ada peringkat
- BMC Neurology: Epidemiology of Childhood Guillan-Barre Syndrome in The North West of IranDokumen5 halamanBMC Neurology: Epidemiology of Childhood Guillan-Barre Syndrome in The North West of IranismaBelum ada peringkat
- FAQs About JAPANESE ENCEPHALITISDokumen4 halamanFAQs About JAPANESE ENCEPHALITISJessica GlitterBelum ada peringkat
- Outcome in Childhood Guillain-Barré SyndromeDokumen5 halamanOutcome in Childhood Guillain-Barré SyndromechristianFPTBelum ada peringkat
- Review Article: Benign Paroxysmal Positional Vertigo: An Integrated PerspectiveDokumen18 halamanReview Article: Benign Paroxysmal Positional Vertigo: An Integrated PerspectivenurulmaulidyahidayatBelum ada peringkat
- NIH Public Access: Author ManuscriptDokumen12 halamanNIH Public Access: Author ManuscriptadipurnamiBelum ada peringkat
- 1 PBDokumen5 halaman1 PBMegaBelum ada peringkat
- SCIWORA-Spinal Cord Injury Without Radiological Abnormality: Veena Kalra, Sheffali Gulati, Mahesh Kamate and Ajay GargDokumen3 halamanSCIWORA-Spinal Cord Injury Without Radiological Abnormality: Veena Kalra, Sheffali Gulati, Mahesh Kamate and Ajay GargnsatriotomoBelum ada peringkat
- A Compilation of Cellular and Tissue Xenotransplantation Studies (1838-2022): A Promising Approach for the Treatment of DiseasesDari EverandA Compilation of Cellular and Tissue Xenotransplantation Studies (1838-2022): A Promising Approach for the Treatment of DiseasesBelum ada peringkat
- Mastery Question MDFDokumen66 halamanMastery Question MDFshaaish100% (1)
- Social Pragmatic Deficits Checklist Sample For Preschool ChildrenDokumen5 halamanSocial Pragmatic Deficits Checklist Sample For Preschool ChildrenBianca GonzalesBelum ada peringkat
- Abscess Incision and Drainage NEJMDokumen4 halamanAbscess Incision and Drainage NEJMMarcela CharryBelum ada peringkat
- Greening The Roadmap of The Philippine Pulp and Paper IndustryDokumen14 halamanGreening The Roadmap of The Philippine Pulp and Paper IndustryJade LimbagoBelum ada peringkat
- Preeclampsia and Severe Preeclampsia GuidelineDokumen10 halamanPreeclampsia and Severe Preeclampsia GuidelineAcitta Raras WimalaBelum ada peringkat
- BasicsOfRadiopharmacy PDFDokumen205 halamanBasicsOfRadiopharmacy PDFFithriana RachmawatiBelum ada peringkat
- Neuro DMS3 FDokumen142 halamanNeuro DMS3 FVicente CáceresBelum ada peringkat
- Dispelling Myths About Drinking Distilled WaterDokumen6 halamanDispelling Myths About Drinking Distilled WaterPau StraitBelum ada peringkat
- Ed GeinDokumen4 halamanEd GeinDaniel OxendineBelum ada peringkat
- 19 Nov Malam Qara Fatikha FixDokumen9 halaman19 Nov Malam Qara Fatikha FixatikahBelum ada peringkat
- Chapter 70-GuytonDokumen9 halamanChapter 70-Guytonswoljaswol1Belum ada peringkat
- Updates in The Treatment of Eating Disorders in 2022 A Year in Review in Eating Disorders The Journal of Treatment PreventionDokumen12 halamanUpdates in The Treatment of Eating Disorders in 2022 A Year in Review in Eating Disorders The Journal of Treatment PreventionMarietta_MonariBelum ada peringkat
- Dr. Suryono, SPJPDokumen26 halamanDr. Suryono, SPJPPowool LalaBelum ada peringkat
- 2016 2017 VHSL Physical FormDokumen4 halaman2016 2017 VHSL Physical FormShreya IyerBelum ada peringkat
- Malaysian Triage CategoryDokumen3 halamanMalaysian Triage CategoryHafiz Hamidi71% (7)
- CWS Lagoons MBR SystemsDokumen3 halamanCWS Lagoons MBR SystemsZoran DespotovicBelum ada peringkat
- MarijuanaDokumen8 halamanMarijuanajohnkyleBelum ada peringkat
- The Deer Exercise For MenDokumen3 halamanThe Deer Exercise For Menkbarn389100% (2)
- Yakeley 2018 Psychoanalysis in Modern Mental Health PracticeDokumen8 halamanYakeley 2018 Psychoanalysis in Modern Mental Health PracticeJonathan RiveraBelum ada peringkat
- Homoeopathic Treatment of Parkinson DieseDokumen23 halamanHomoeopathic Treatment of Parkinson DieseNidhi SrivastavaBelum ada peringkat
- Ii 2015 1Dokumen266 halamanIi 2015 1tuni santeBelum ada peringkat
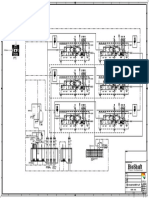
- P&ID - STP-Yanbu SWCC (6units)Dokumen1 halamanP&ID - STP-Yanbu SWCC (6units)Ashraf BayomiBelum ada peringkat
- Antenatal Diet PlanDokumen7 halamanAntenatal Diet PlanSunija Selvam100% (3)
- EpulisDokumen7 halamanEpulisSean Anderson100% (1)
- Tetralogy Hypercyanotic SpellDokumen3 halamanTetralogy Hypercyanotic SpellJunior PratasikBelum ada peringkat
- 52 Healing HabitsDokumen11 halaman52 Healing Habitsjethro123_69Belum ada peringkat
- Guidance ServicesDokumen56 halamanGuidance Servicesminna comuyogBelum ada peringkat
- Resource - Initial Assessment TemplateDokumen7 halamanResource - Initial Assessment TemplateHarram SajjadBelum ada peringkat
- Moot Court BrochureDokumen16 halamanMoot Court BrochureAkashBelum ada peringkat
- Jurnal SkoliosisDokumen9 halamanJurnal SkoliosisLidya SiahaanBelum ada peringkat