Anda mungkin juga menyukai
- Advanced Life Support Questions - Answers PaperDokumen5 halamanAdvanced Life Support Questions - Answers Paperjahangirealam50% (10)
- Final FRCA Viva Questions From June 2011 Exam Some General Feedback For The Day For Any Future CandidatesDokumen56 halamanFinal FRCA Viva Questions From June 2011 Exam Some General Feedback For The Day For Any Future Candidatesjahangirealam89% (9)
- MEDACS ReferenceDokumen3 halamanMEDACS ReferencejahangirealamBelum ada peringkat
- Principles of Medication AdministrationDokumen13 halamanPrinciples of Medication Administrationloujille89% (9)
- Scars & Devices in Paces 4th Edition PDFDokumen132 halamanScars & Devices in Paces 4th Edition PDFKaleem Ullah Bhatti100% (2)
- Bojar PediatricDokumen123 halamanBojar PediatricLuqman AlwiBelum ada peringkat
- Cardiovascular DisorderDokumen88 halamanCardiovascular DisorderSandeepBelum ada peringkat
- Preoperative AssessmentDokumen24 halamanPreoperative AssessmentjahangirealamBelum ada peringkat
- Septic Shock: Submitted By: Chezka Marie R. Palola NRPP Batch 55Dokumen4 halamanSeptic Shock: Submitted By: Chezka Marie R. Palola NRPP Batch 55Chezka PalolaBelum ada peringkat
- Congenital Heart Diseases.Dokumen86 halamanCongenital Heart Diseases.Salman KhanBelum ada peringkat
- Hypoplastic Left Heart SyndromeDokumen13 halamanHypoplastic Left Heart SyndromeYaser AlmafrajiBelum ada peringkat
- Children: The Pulmonary Circulation in The Single Ventricle PatientDokumen12 halamanChildren: The Pulmonary Circulation in The Single Ventricle PatientFernando PinedaBelum ada peringkat
- Aruna Ramesh-Emergency...Dokumen6 halamanAruna Ramesh-Emergency...Aishu BBelum ada peringkat
- Fetal Perfusion/Congenital Heart DefectsDokumen13 halamanFetal Perfusion/Congenital Heart DefectsMatthew RyanBelum ada peringkat
- Tetralogy of FallotDokumen7 halamanTetralogy of FallotWidelmark FarrelBelum ada peringkat
- What Is Tetralogy of FallotDokumen18 halamanWhat Is Tetralogy of FallotIyah Bu-ucanBelum ada peringkat
- Transposition of Great ArteriesDokumen18 halamanTransposition of Great Arteriesparmeshori100% (2)
- Management of Persistent Ductus ArteriosusDokumen79 halamanManagement of Persistent Ductus Arteriosushashim adekunleBelum ada peringkat
- Congenital Heart DiseaseDokumen20 halamanCongenital Heart DiseaseMahdi AlattasBelum ada peringkat
- Approach To A Child With Congenital Heart DiseaseDokumen31 halamanApproach To A Child With Congenital Heart DiseaseMUHAMMAD DANIAL BIN HASAN FPSKBelum ada peringkat
- Lapkas Pediatrik NLDokumen31 halamanLapkas Pediatrik NLHannaTashiaClaudiaBelum ada peringkat
- Heart Disease and PregnancyDokumen7 halamanHeart Disease and PregnancyBagus Wanda HabibullahBelum ada peringkat
- Tetralogy of Fallot PDFDokumen11 halamanTetralogy of Fallot PDFIma SoniaBelum ada peringkat
- Aortopulmonary Window in InfantsDokumen3 halamanAortopulmonary Window in Infantsonlyjust4meBelum ada peringkat
- Intervento Di FontaneDokumen3 halamanIntervento Di FontaneJ.c. ColussusBelum ada peringkat
- J Am Heart Assoc 2014 NannaDokumen19 halamanJ Am Heart Assoc 2014 NannaBagus Wanda HabibullahBelum ada peringkat
- Tricuspid AtresiaDokumen44 halamanTricuspid Atresiadoctorsaty7539Belum ada peringkat
- Valvular Heart Disease in Pregnancy: Review ArticleDokumen13 halamanValvular Heart Disease in Pregnancy: Review ArticleGlenn Alend Wowor GlennBelum ada peringkat
- OB EmbolismDokumen31 halamanOB EmbolismAbigail Hazel Patiño NaveaBelum ada peringkat
- DR Varsha Atul Shah Senior Consultant Dept of Neonatal and Devt Medicine, SGH Visiting Consultant Dept of Child Devt, KKHDokumen47 halamanDR Varsha Atul Shah Senior Consultant Dept of Neonatal and Devt Medicine, SGH Visiting Consultant Dept of Child Devt, KKHJennifer MrjBelum ada peringkat
- Heart Disease and PregnancyDokumen6 halamanHeart Disease and PregnancyBagus Wanda Habibullah100% (1)
- Cardiovascular Disorders: Prepared By: Wad-Ey, Rosie Glae, RNDokumen49 halamanCardiovascular Disorders: Prepared By: Wad-Ey, Rosie Glae, RNrosieglaeBelum ada peringkat
- Tetralogy of FallotDokumen5 halamanTetralogy of FallotSaloni MehtaBelum ada peringkat
- Congenital Heart Defect-VsdDokumen53 halamanCongenital Heart Defect-VsdAuni Akif AleesaBelum ada peringkat
- Heart Failure in Adult Congenital Heart Disease Nonpharmacologic Treatment StrategiesDokumen10 halamanHeart Failure in Adult Congenital Heart Disease Nonpharmacologic Treatment StrategiesAndhika DBelum ada peringkat
- Bab 20 TambahanDokumen3 halamanBab 20 TambahanNur SulistiyaningsihBelum ada peringkat
- Congenital Heart Disease (2011)Dokumen17 halamanCongenital Heart Disease (2011)drheay100% (1)
- Amniotic Fluid Embolism ArticleDokumen3 halamanAmniotic Fluid Embolism ArticleShailesh JainBelum ada peringkat
- Anesthesia For Non Cardiac Surgery in Children With Congenital Heart DiseaseDokumen3 halamanAnesthesia For Non Cardiac Surgery in Children With Congenital Heart Diseasevenkatesh chowdaryBelum ada peringkat
- Nursing Acn-IiDokumen80 halamanNursing Acn-IiMunawar100% (6)
- Fetal Cardiac Intervention Rational, Risk and BenefitDokumen4 halamanFetal Cardiac Intervention Rational, Risk and BenefitThomson AffendyBelum ada peringkat
- Frommelt 2014Dokumen12 halamanFrommelt 2014Nestor FerrerBelum ada peringkat
- Doppler en ObstetriciaDokumen8 halamanDoppler en Obstetriciapopman41Belum ada peringkat
- Current Concepts in Fetal CV Disease - CLPDokumen19 halamanCurrent Concepts in Fetal CV Disease - CLPSridhar KaushikBelum ada peringkat
- Pathophysiology of Birth AsphyxiaDokumen14 halamanPathophysiology of Birth AsphyxiaEduardo Rios DuboisBelum ada peringkat
- Poster Presentation CCRA Malang 2014Dokumen3 halamanPoster Presentation CCRA Malang 2014alfarobi yogiBelum ada peringkat
- Duct Dependent Heart Lesions by DR Parashuram Waddar (Pediatrician, MBBS, DCH DNB)Dokumen63 halamanDuct Dependent Heart Lesions by DR Parashuram Waddar (Pediatrician, MBBS, DCH DNB)parasuram waddarBelum ada peringkat
- Presented by DR Rahul D AgrawalDokumen64 halamanPresented by DR Rahul D AgrawalRahul AgrawalBelum ada peringkat
- Stenosis Pulmonal.Dokumen21 halamanStenosis Pulmonal.syelBelum ada peringkat
- Hollamby Mitchell s5001226 Case 1 DtgaDokumen13 halamanHollamby Mitchell s5001226 Case 1 Dtgaapi-299009880Belum ada peringkat
- Tamizaje Enfermedades CardiacasDokumen16 halamanTamizaje Enfermedades CardiacasDanna GonzálezBelum ada peringkat
- Pediatric Patent Ductus ArteriosusDokumen12 halamanPediatric Patent Ductus Arteriosusabirami_murugesuBelum ada peringkat
- Echocardiographic Evaluation of Tetralogy of Fallot : Echo in Adult Congenital Heart DiseaseDokumen9 halamanEchocardiographic Evaluation of Tetralogy of Fallot : Echo in Adult Congenital Heart DiseaseResiden KardiologiBelum ada peringkat
- HydropsDokumen13 halamanHydropsalejandro1122Belum ada peringkat
- Mitral Stenosis For Non-Cardiac Surgery Case FileDokumen4 halamanMitral Stenosis For Non-Cardiac Surgery Case Filehttps://medical-phd.blogspot.comBelum ada peringkat
- Tof Case ReportDokumen11 halamanTof Case ReportPatrick DycocoBelum ada peringkat
- Pulmonary Atresia With Ventricular Septal Defect: Systematic ReviewDokumen10 halamanPulmonary Atresia With Ventricular Septal Defect: Systematic ReviewIvan VeriswanBelum ada peringkat
- Aiims - Pediatrics Q&ADokumen207 halamanAiims - Pediatrics Q&AqqypprcyxyBelum ada peringkat
- Esophageal Varices: Pathophysiology, Approach, and Clinical DilemmasDokumen2 halamanEsophageal Varices: Pathophysiology, Approach, and Clinical Dilemmaskaychi zBelum ada peringkat
- Down Syndrome: Case ReportsDokumen4 halamanDown Syndrome: Case ReportsPedro CardosoBelum ada peringkat
- Pleural Effusion in Adults-Etiology, Diagnosis, and Treatment (24.05.2019)Dokumen10 halamanPleural Effusion in Adults-Etiology, Diagnosis, and Treatment (24.05.2019)lordiroh1Belum ada peringkat
- Cardiovascular System Dr. Eman Badr 2020Dokumen182 halamanCardiovascular System Dr. Eman Badr 2020Amina DinarBelum ada peringkat
- Herberg 2014Dokumen8 halamanHerberg 2014ANA HERNÁNDEZBelum ada peringkat
- USC Moe FINAL - SV PhysiologyDokumen5 halamanUSC Moe FINAL - SV PhysiologyindahBelum ada peringkat
- Neonatal Circulation Changes / Unbalanced Circulation: Neonatal Cardiac Conditions: Medical and Surgical ManagementDokumen4 halamanNeonatal Circulation Changes / Unbalanced Circulation: Neonatal Cardiac Conditions: Medical and Surgical ManagementAnita Maria UlfaBelum ada peringkat
- Tetralogy of FallotDokumen28 halamanTetralogy of FallotconcozBelum ada peringkat
- Acute Stridor in Children CA1080 v.8Dokumen13 halamanAcute Stridor in Children CA1080 v.8jahangirealamBelum ada peringkat
- 426-288-18DD-A - Job Description Specialty Doctor August 2018Dokumen11 halaman426-288-18DD-A - Job Description Specialty Doctor August 2018jahangirealamBelum ada peringkat
- Applied IM & FM Programs 2018Dokumen269 halamanApplied IM & FM Programs 2018jahangirealamBelum ada peringkat
- Cam PDFDokumen13 halamanCam PDFjahangirealamBelum ada peringkat
- Specialty Doctor in ICU and Anaesthetics Job Description: East and North Hertfordshire NHS TrustDokumen20 halamanSpecialty Doctor in ICU and Anaesthetics Job Description: East and North Hertfordshire NHS TrustjahangirealamBelum ada peringkat
- Support Staff Employment Application Form September 2017.122288453Dokumen10 halamanSupport Staff Employment Application Form September 2017.122288453jahangirealamBelum ada peringkat
- Find Multiples of 2Dokumen1 halamanFind Multiples of 2jahangirealamBelum ada peringkat
- I FoundationsDokumen7 halamanI FoundationsjahangirealamBelum ada peringkat
- Dla1a Child PrintDokumen61 halamanDla1a Child PrintjahangirealamBelum ada peringkat
- Obstructive Sleep Apnoea and AnaesthesiaDokumen21 halamanObstructive Sleep Apnoea and AnaesthesiajahangirealamBelum ada peringkat
- Duplicate Copy: Balance Due 123001.08Dokumen2 halamanDuplicate Copy: Balance Due 123001.08jahangirealamBelum ada peringkat
- Baromtric (89 Pages)Dokumen89 halamanBaromtric (89 Pages)jahangirealamBelum ada peringkat
- Bier Block (Intravenous Regional Anesthesia), Handout PDFDokumen8 halamanBier Block (Intravenous Regional Anesthesia), Handout PDFjahangirealamBelum ada peringkat
- NHS Lothian Medical Application FormDokumen17 halamanNHS Lothian Medical Application FormjahangirealamBelum ada peringkat
- Dress Up As... : The GruffaloDokumen4 halamanDress Up As... : The GruffalojahangirealamBelum ada peringkat
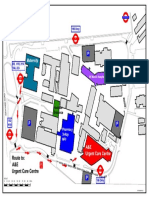
- NPHNew Wayfinding V6Dokumen1 halamanNPHNew Wayfinding V6jahangirealamBelum ada peringkat
- List of OSCE Stations in Past Six Months in PLAB Part 2 PLAB Part 2Dokumen12 halamanList of OSCE Stations in Past Six Months in PLAB Part 2 PLAB Part 2jahangirealam100% (1)
- Application SummaryDokumen3 halamanApplication SummaryjahangirealamBelum ada peringkat
- Acute: Renal Failure Management in The NeonateDokumen8 halamanAcute: Renal Failure Management in The NeonatejahangirealamBelum ada peringkat
- Introduction To Clinical TrialsDokumen9 halamanIntroduction To Clinical Trialsmuhammad murtazaBelum ada peringkat
- Gus156 Slide Ginjal Dan Saluran KemihDokumen128 halamanGus156 Slide Ginjal Dan Saluran KemihRina ChairunnisaBelum ada peringkat
- ACUTE RESPIRATORY FAILURE QuizDokumen3 halamanACUTE RESPIRATORY FAILURE QuizTrish 001950% (2)
- Out 8Dokumen10 halamanOut 8tofanBelum ada peringkat
- Advocacy Letter-Amy JohnsDokumen2 halamanAdvocacy Letter-Amy Johnsapi-239145075Belum ada peringkat
- Shibly Rahman PacesDokumen356 halamanShibly Rahman PacesMohammadAbdurRahmanBelum ada peringkat
- Time Table Cardiology: Da y Date Topic Learning Situation English Class Regular Class PICDokumen5 halamanTime Table Cardiology: Da y Date Topic Learning Situation English Class Regular Class PICSheryl ElitaBelum ada peringkat
- Blood Transfusion, BERNABE, LAWRA MAE E. BSN2-BDokumen2 halamanBlood Transfusion, BERNABE, LAWRA MAE E. BSN2-BLaw MaeBelum ada peringkat
- Community Acquired PneumoniaDokumen56 halamanCommunity Acquired Pneumoniashiean06Belum ada peringkat
- Claim Form - HospitalizationDokumen8 halamanClaim Form - HospitalizationNishantShah100% (1)
- Practice Test Questions Downloaded From FILIPINO NURSES CENTRALDokumen4 halamanPractice Test Questions Downloaded From FILIPINO NURSES CENTRALFilipino Nurses CentralBelum ada peringkat
- Newborn Thesis Neel Kamal 102802004Dokumen105 halamanNewborn Thesis Neel Kamal 102802004Prabir Kumar ChatterjeeBelum ada peringkat
- Messy Purse Girls - Women and ADHDDokumen5 halamanMessy Purse Girls - Women and ADHDgramarina100% (7)
- System: Total Solution For Value-Based Healthcare PurchasingDokumen17 halamanSystem: Total Solution For Value-Based Healthcare PurchasingmochkurniawanBelum ada peringkat
- National Tuberculosis Control Program: Dr. Kanupriya ChaturvediDokumen37 halamanNational Tuberculosis Control Program: Dr. Kanupriya ChaturvediAlyn Paul EmnacenBelum ada peringkat
- Guiding For HospitalDokumen14 halamanGuiding For HospitalAnkit Bhatia100% (1)
- Ludwig's AnginaDokumen2 halamanLudwig's AnginaegyseptiansyahBelum ada peringkat
- Rheumatic Heart Disease PathophysiologyDokumen3 halamanRheumatic Heart Disease Pathophysiologyjethro sanchez100% (1)
- IV Fluid Replacement TherapyDokumen12 halamanIV Fluid Replacement TherapyKamran Sheraz100% (1)
- Sympathomimetic DrugsDokumen4 halamanSympathomimetic DrugsKardo WeedBelum ada peringkat
- 89 12 08 Bazamozi Markaz Behdasht Diagnosis of TBDokumen45 halaman89 12 08 Bazamozi Markaz Behdasht Diagnosis of TBvijaya_vijju_1586982Belum ada peringkat
- SUPPORT Doctor Letter of Support - BognerDokumen6 halamanSUPPORT Doctor Letter of Support - BognerKen WolskiBelum ada peringkat
- Probiotics in Diarrhea PDFDokumen5 halamanProbiotics in Diarrhea PDFShankar YadavBelum ada peringkat
- Referat DR IhsanilDokumen9 halamanReferat DR IhsanilmerahdanmerahBelum ada peringkat
- Orientation Jaw RelationDokumen11 halamanOrientation Jaw RelationHoney AroraBelum ada peringkat
- Edkt 2030-Graded DiscussionDokumen2 halamanEdkt 2030-Graded Discussionapi-271964727Belum ada peringkat
- Potts DiseaseDokumen3 halamanPotts DiseasePaul Stephen PinedaBelum ada peringkat