Anda mungkin juga menyukai
- Orthopaedic Management in Cerebral Palsy, 2nd EditionDari EverandOrthopaedic Management in Cerebral Palsy, 2nd EditionHelen Meeks HorstmannPenilaian: 3 dari 5 bintang3/5 (2)
- Module 10 Upper Extremity FINAL 16edDokumen163 halamanModule 10 Upper Extremity FINAL 16edgialinuBelum ada peringkat
- Functional Rehabilitation of Some Common Neurological Conditions: A Physical Management Strategy to Optimise Functional Activity LevelDari EverandFunctional Rehabilitation of Some Common Neurological Conditions: A Physical Management Strategy to Optimise Functional Activity LevelBelum ada peringkat
- Chapter 10 Upper Extremity Interventions PDFDokumen208 halamanChapter 10 Upper Extremity Interventions PDFRonny Méndez VasconcellosBelum ada peringkat
- Motor and Proprioception Deficits in Post Rehab StrokeDokumen21 halamanMotor and Proprioception Deficits in Post Rehab StrokeApril Bramhall EddyBelum ada peringkat
- Sensory Re-Education: Hand Physiotherapy DepartmentDokumen2 halamanSensory Re-Education: Hand Physiotherapy DepartmentEmanuel George StoenescuBelum ada peringkat
- Evaluation of The Hand!Dokumen84 halamanEvaluation of The Hand!Ahmad A. Fannoon100% (1)
- Neurological ExaminationDokumen13 halamanNeurological Examinationsaveetha purushothamanBelum ada peringkat
- EBRSR Handbook Chapter 4 - Upper Extremity Post Stroke - MLDokumen60 halamanEBRSR Handbook Chapter 4 - Upper Extremity Post Stroke - MLanjelikaBelum ada peringkat
- FIM ManualDokumen24 halamanFIM ManualAnshuman MihirBelum ada peringkat
- Orthosisofhandppt 181202162551Dokumen65 halamanOrthosisofhandppt 181202162551Khageswar SamalBelum ada peringkat
- Bobath Approach Concepts and Principles: by DR - Shahid Shabbir DPT, Ms - NMPTDokumen21 halamanBobath Approach Concepts and Principles: by DR - Shahid Shabbir DPT, Ms - NMPTrabia khalid100% (1)
- Introduction To MovementsDokumen42 halamanIntroduction To MovementsRamalingam KanagarajBelum ada peringkat
- Rubric Mini PracticalDokumen2 halamanRubric Mini PracticalAigen OcampoBelum ada peringkat
- Part 2: Social Skills Training: RatingDokumen3 halamanPart 2: Social Skills Training: RatingGina GucioBelum ada peringkat
- Classification of Upper Limb OrthosesDokumen16 halamanClassification of Upper Limb Orthoseszoha hassanBelum ada peringkat
- Execution Function Perfor Test PDFDokumen21 halamanExecution Function Perfor Test PDFLydia MartínBelum ada peringkat
- Tetraplegia Hand Activity QuestionnaireDokumen20 halamanTetraplegia Hand Activity QuestionnaireISLinkBelum ada peringkat
- SCALE-Selective Control Assesment PDFDokumen3 halamanSCALE-Selective Control Assesment PDFjinil raj j.r.Belum ada peringkat
- Exit Project Workbook Complete Draft 2Dokumen2 halamanExit Project Workbook Complete Draft 2vladBelum ada peringkat
- Pediatric Wheelchair Toolkit FINALDokumen6 halamanPediatric Wheelchair Toolkit FINALIndiana Family to FamilyBelum ada peringkat
- Chapter 8Dokumen30 halamanChapter 8Karla CarazoBelum ada peringkat
- Motor MildstonesDokumen13 halamanMotor MildstonesVaio Wolff AbendrothBelum ada peringkat
- Assessment of HandDokumen76 halamanAssessment of Handchirag0% (1)
- OT - Milestone RetypedDokumen6 halamanOT - Milestone RetypedAubrey Vale SagunBelum ada peringkat
- Lateral Epicondylitis - Tennis Ellbow HandoutDokumen5 halamanLateral Epicondylitis - Tennis Ellbow Handoutgermany23Belum ada peringkat
- Rood Approach Muscle RehabilitationDokumen33 halamanRood Approach Muscle RehabilitationCedricFernandez100% (1)
- Ataxias Neuro Condition DetailedDokumen80 halamanAtaxias Neuro Condition DetailedMikail AtiyehBelum ada peringkat
- Hip Displacement in Cerebral PalsyDokumen9 halamanHip Displacement in Cerebral PalsyJohannesSchoppmannBelum ada peringkat
- Wolf Motor Function TestDokumen23 halamanWolf Motor Function TestSai RamBelum ada peringkat
- Vojta Therapy: Reflex Creeping in A Prone Lying Position and Reflex Rolling From A Supine and Side LyingDokumen7 halamanVojta Therapy: Reflex Creeping in A Prone Lying Position and Reflex Rolling From A Supine and Side LyingSonali SoumyashreeBelum ada peringkat
- Effect of Parent-Delivered Action Observation Therapy On Upper Limb Function in Unilateral Cerebral PalsyDokumen40 halamanEffect of Parent-Delivered Action Observation Therapy On Upper Limb Function in Unilateral Cerebral PalsyNovaria Puspita SamudraBelum ada peringkat
- Neuro-Developmental Clinical ObservationsDokumen2 halamanNeuro-Developmental Clinical ObservationsAmitesh NarayanBelum ada peringkat
- Cerebral PalsyDokumen23 halamanCerebral Palsyane2sa100% (1)
- What Is Spinal Cord InjuryDokumen20 halamanWhat Is Spinal Cord Injurymizah100% (1)
- Adult Psychiatric Sensory Integration EvaluationDokumen18 halamanAdult Psychiatric Sensory Integration Evaluationemesep1850% (2)
- Muscle Grading and Testing ProceduresDokumen5 halamanMuscle Grading and Testing Proceduresshodhganga100% (1)
- GWS Total Hip ReplacementDokumen17 halamanGWS Total Hip ReplacementRadu MoglanBelum ada peringkat
- Shoulder Impingement GuidelinesDokumen3 halamanShoulder Impingement GuidelinesTasha MillerBelum ada peringkat
- Ot Guidelines ParkinsonDokumen145 halamanOt Guidelines ParkinsonFannyBelum ada peringkat
- Stroke Rehab, Info Proving PNF To Improve Upper Limb Function - FullDokumen6 halamanStroke Rehab, Info Proving PNF To Improve Upper Limb Function - FullThomas CorbettBelum ada peringkat
- Nuero RehabDokumen14 halamanNuero RehabLINDSLEY GOBelum ada peringkat
- OT8 - Thumb Immobilization SplintDokumen4 halamanOT8 - Thumb Immobilization SplintAnnbe Barte100% (1)
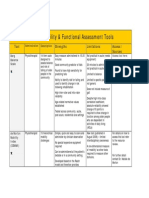
- Assessment Tools for Mobility & Functional IndependenceDokumen4 halamanAssessment Tools for Mobility & Functional Independencesonya63265Belum ada peringkat
- MGH Wrist and Elbow Strengthening ExercisesDokumen1 halamanMGH Wrist and Elbow Strengthening ExercisesRidwan Hadinata SalimBelum ada peringkat
- Design of A Hand OrthosisDokumen251 halamanDesign of A Hand OrthosisIsrael BlancoBelum ada peringkat
- Orthopedic Physiotherapy Assignment: 1. Patient HistoryDokumen4 halamanOrthopedic Physiotherapy Assignment: 1. Patient HistoryarushiBelum ada peringkat
- Gait in Children With Cerebral PalsyDokumen5 halamanGait in Children With Cerebral PalsyvarahamihirBelum ada peringkat
- Development Chart For BookletDokumen13 halamanDevelopment Chart For BookletzapelBelum ada peringkat
- OT 460 Intervention Kit AssignmentDokumen2 halamanOT 460 Intervention Kit AssignmentMegan McCarthyBelum ada peringkat
- Rehabilitation Priciples at Children With Cerebral Palsy After NDT Bobath ConceptDokumen13 halamanRehabilitation Priciples at Children With Cerebral Palsy After NDT Bobath ConceptAndrei TîrziuBelum ada peringkat
- Mirror Box Presentation Handout EditedDokumen4 halamanMirror Box Presentation Handout Editedapi-364398898Belum ada peringkat
- Sitbat 16item FinalDokumen6 halamanSitbat 16item FinalMae NocheBelum ada peringkat
- Amputee Activity Score PDFDokumen5 halamanAmputee Activity Score PDFLydia MartínBelum ada peringkat
- Stroke UE ToolkitDokumen69 halamanStroke UE ToolkitWhitney JosephBelum ada peringkat
- Tactile Defensiveness PDFDokumen7 halamanTactile Defensiveness PDFCristi BacuBelum ada peringkat
- Sensory Diet Handout for Developmental FXDokumen7 halamanSensory Diet Handout for Developmental FXpratibhaumrariya100% (1)
- 4.sensorry ExaminationDokumen27 halaman4.sensorry Examinationtalha malikBelum ada peringkat
- 4.sensorry ExaminationDokumen27 halaman4.sensorry ExaminationSalman KhanBelum ada peringkat
- Module 7 Techniques in Physical AssessmentDokumen14 halamanModule 7 Techniques in Physical AssessmentCalvo AdrianBelum ada peringkat
- Sotai ExercisesDokumen2 halamanSotai Exerciseskokobamba100% (4)
- MEDUMAT Standard 2 83700-ENDokumen16 halamanMEDUMAT Standard 2 83700-ENJagath PrasangaBelum ada peringkat
- 13 Other Blood Group SystemsDokumen56 halaman13 Other Blood Group SystemsCarinaJongLeeBelum ada peringkat
- Stress Management in StudentsDokumen25 halamanStress Management in StudentsJangBelum ada peringkat
- Drug Development and BEDokumen19 halamanDrug Development and BEJoseph KamaleshBelum ada peringkat
- Anorectal MalformationDokumen40 halamanAnorectal Malformationblessy83% (18)
- Anc 0001 0009 0151Dokumen42 halamanAnc 0001 0009 0151ManhaBelum ada peringkat
- Aesthetic Jurnal PDFDokumen20 halamanAesthetic Jurnal PDFTarrayuanaBelum ada peringkat
- Q1 Grade 10 HEALTH DLL Week 2Dokumen14 halamanQ1 Grade 10 HEALTH DLL Week 2Leonor MayoyaBelum ada peringkat
- Renal Disease Dental ManagmentDokumen25 halamanRenal Disease Dental ManagmentPratyusha VallamBelum ada peringkat
- Reaserch PaperDokumen9 halamanReaserch PaperMridul NigamBelum ada peringkat
- General Introduction To AcupointsDokumen48 halamanGeneral Introduction To Acupointsjonan hemingted10Belum ada peringkat
- Medium Opening Activator: (Removable Functional Appliance)Dokumen22 halamanMedium Opening Activator: (Removable Functional Appliance)Abiha AliBelum ada peringkat
- Do Clear Cell Ovarian Carcinomas Have Poorer Prognosis Compared To Other Epithelial Cell Types? A Study of 1411 Clear Cell Ovarian CancersDokumen7 halamanDo Clear Cell Ovarian Carcinomas Have Poorer Prognosis Compared To Other Epithelial Cell Types? A Study of 1411 Clear Cell Ovarian CancersNi Wayan Ana PsBelum ada peringkat
- 2 05MasteringMBBRprocessdesignforcarbonandnitrogenabatementDokumen65 halaman2 05MasteringMBBRprocessdesignforcarbonandnitrogenabatementYên BìnhBelum ada peringkat
- English Language f1 2013 Mid YearDokumen7 halamanEnglish Language f1 2013 Mid YearSiti ZawiyahBelum ada peringkat
- Baseline Evaluation and Management of RetinoblastomaDokumen19 halamanBaseline Evaluation and Management of RetinoblastomaSiddharth KatyalBelum ada peringkat
- Dramatizing Dementia: Madness in The Plays of Tennessee WilliamsDokumen8 halamanDramatizing Dementia: Madness in The Plays of Tennessee WilliamsMarcusFelsmanBelum ada peringkat
- PTRDokumen8 halamanPTRRaj VillarinBelum ada peringkat
- February 4, 2015Dokumen12 halamanFebruary 4, 2015The Delphos HeraldBelum ada peringkat
- Material Safety Data Sheet: Product and Company Identification 1Dokumen6 halamanMaterial Safety Data Sheet: Product and Company Identification 1onejako12Belum ada peringkat
- History of PenicillinDokumen3 halamanHistory of PenicillinJhunel Antonio RomanBelum ada peringkat
- Atomoxetine in ADHD in Children With and Without Comorbid Mood DisordersDokumen10 halamanAtomoxetine in ADHD in Children With and Without Comorbid Mood DisordersNeuro GYMBelum ada peringkat
- Euro J of Neurology - 2021 - Van Den Bergh - European Academy of Neurology Peripheral Nerve Society Guideline On DiagnosisDokumen28 halamanEuro J of Neurology - 2021 - Van Den Bergh - European Academy of Neurology Peripheral Nerve Society Guideline On DiagnosisSusana RocheBelum ada peringkat
- HypertensionDokumen39 halamanHypertensiontianallyBelum ada peringkat
- Surgical Approaches To The Skull BaseDokumen2 halamanSurgical Approaches To The Skull Baseİbrahim ErkutluBelum ada peringkat
- Motion SicknessDokumen5 halamanMotion SicknessIbrahim AbdullahBelum ada peringkat
- Cytokines - IntroductionDokumen2 halamanCytokines - IntroductionTra gicBelum ada peringkat
- Rotator CuffDokumen46 halamanRotator Cuffeuan00Belum ada peringkat
- Bmet 262 Outline 2022 2023Dokumen12 halamanBmet 262 Outline 2022 2023Emmanuel PrahBelum ada peringkat
- Weapons of Mass Instruction: A Schoolteacher's Journey Through the Dark World of Compulsory SchoolingDari EverandWeapons of Mass Instruction: A Schoolteacher's Journey Through the Dark World of Compulsory SchoolingPenilaian: 4.5 dari 5 bintang4.5/5 (149)
- Summary: The 5AM Club: Own Your Morning. Elevate Your Life. by Robin Sharma: Key Takeaways, Summary & AnalysisDari EverandSummary: The 5AM Club: Own Your Morning. Elevate Your Life. by Robin Sharma: Key Takeaways, Summary & AnalysisPenilaian: 4.5 dari 5 bintang4.5/5 (22)
- How to Talk to Anyone: Learn the Secrets of Good Communication and the Little Tricks for Big Success in RelationshipDari EverandHow to Talk to Anyone: Learn the Secrets of Good Communication and the Little Tricks for Big Success in RelationshipPenilaian: 4.5 dari 5 bintang4.5/5 (1135)
- The 16 Undeniable Laws of Communication: Apply Them and Make the Most of Your MessageDari EverandThe 16 Undeniable Laws of Communication: Apply Them and Make the Most of Your MessagePenilaian: 5 dari 5 bintang5/5 (72)
- Summary: Greenlights: by Matthew McConaughey: Key Takeaways, Summary & AnalysisDari EverandSummary: Greenlights: by Matthew McConaughey: Key Takeaways, Summary & AnalysisPenilaian: 4 dari 5 bintang4/5 (6)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisDari EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisPenilaian: 5 dari 5 bintang5/5 (3)
- Summary: I'm Glad My Mom Died: by Jennette McCurdy: Key Takeaways, Summary & AnalysisDari EverandSummary: I'm Glad My Mom Died: by Jennette McCurdy: Key Takeaways, Summary & AnalysisPenilaian: 4.5 dari 5 bintang4.5/5 (2)
- Summary: The Laws of Human Nature: by Robert Greene: Key Takeaways, Summary & AnalysisDari EverandSummary: The Laws of Human Nature: by Robert Greene: Key Takeaways, Summary & AnalysisPenilaian: 4.5 dari 5 bintang4.5/5 (30)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4.5 dari 5 bintang4.5/5 (1871)
- Dumbing Us Down: The Hidden Curriculum of Compulsory SchoolingDari EverandDumbing Us Down: The Hidden Curriculum of Compulsory SchoolingPenilaian: 4.5 dari 5 bintang4.5/5 (495)
- Make It Stick by Peter C. Brown, Henry L. Roediger III, Mark A. McDaniel - Book Summary: The Science of Successful LearningDari EverandMake It Stick by Peter C. Brown, Henry L. Roediger III, Mark A. McDaniel - Book Summary: The Science of Successful LearningPenilaian: 4.5 dari 5 bintang4.5/5 (55)
- Financial Feminist: Overcome the Patriarchy's Bullsh*t to Master Your Money and Build a Life You LoveDari EverandFinancial Feminist: Overcome the Patriarchy's Bullsh*t to Master Your Money and Build a Life You LovePenilaian: 5 dari 5 bintang5/5 (1)
- The Story of the World, Vol. 2 AudiobookDari EverandThe Story of the World, Vol. 2 AudiobookPenilaian: 5 dari 5 bintang5/5 (1)
- Learn Spanish While SleepingDari EverandLearn Spanish While SleepingPenilaian: 4 dari 5 bintang4/5 (20)
- Summary: Trading in the Zone: Trading in the Zone: Master the Market with Confidence, Discipline, and a Winning Attitude by Mark Douglas: Key Takeaways, Summary & AnalysisDari EverandSummary: Trading in the Zone: Trading in the Zone: Master the Market with Confidence, Discipline, and a Winning Attitude by Mark Douglas: Key Takeaways, Summary & AnalysisPenilaian: 5 dari 5 bintang5/5 (15)
- Learn French While SleepingDari EverandLearn French While SleepingPenilaian: 3 dari 5 bintang3/5 (9)
- Functional Training and Beyond: Building the Ultimate Superfunctional Body and MindDari EverandFunctional Training and Beyond: Building the Ultimate Superfunctional Body and MindPenilaian: 4.5 dari 5 bintang4.5/5 (1)
- Learn Japanese While SleepingDari EverandLearn Japanese While SleepingPenilaian: 5 dari 5 bintang5/5 (5)
- Follow The Leader: A Collection Of The Best Lectures On LeadershipDari EverandFollow The Leader: A Collection Of The Best Lectures On LeadershipPenilaian: 5 dari 5 bintang5/5 (122)
- Little Soldiers: An American Boy, a Chinese School, and the Global Race to AchieveDari EverandLittle Soldiers: An American Boy, a Chinese School, and the Global Race to AchievePenilaian: 4 dari 5 bintang4/5 (25)
- How to Improve English Speaking: How to Become a Confident and Fluent English SpeakerDari EverandHow to Improve English Speaking: How to Become a Confident and Fluent English SpeakerPenilaian: 4.5 dari 5 bintang4.5/5 (56)
- Think Ahead: 7 Decisions You Can Make Today for the God-Honoring Life You Want TomorrowDari EverandThink Ahead: 7 Decisions You Can Make Today for the God-Honoring Life You Want TomorrowPenilaian: 5 dari 5 bintang5/5 (7)
- Whatever It Takes: Geoffrey Canada's Quest to Change Harlem and AmericaDari EverandWhatever It Takes: Geoffrey Canada's Quest to Change Harlem and AmericaPenilaian: 4 dari 5 bintang4/5 (79)
- Summary of The Power of Habit: Why We Do What We Do in Life and Business by Charles DuhiggDari EverandSummary of The Power of Habit: Why We Do What We Do in Life and Business by Charles DuhiggPenilaian: 4.5 dari 5 bintang4.5/5 (261)
- The Story of the World, Vol. 1 AudiobookDari EverandThe Story of the World, Vol. 1 AudiobookPenilaian: 5 dari 5 bintang5/5 (2)
- Weapons of Mass Instruction: A Schoolteacher's Journey Through the Dark World of Compulsory SchoolingDari EverandWeapons of Mass Instruction: A Schoolteacher's Journey Through the Dark World of Compulsory SchoolingPenilaian: 4 dari 5 bintang4/5 (59)