Anda mungkin juga menyukai
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Pathophysiology Chapter 21Dokumen12 halamanPathophysiology Chapter 21Christina100% (6)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- Casestudy UTIDokumen53 halamanCasestudy UTIRuja Shakya100% (3)
- Ayurveda For EveryoneDokumen1 halamanAyurveda For EveryoneSanjay PisharodiBelum ada peringkat
- Ayurvedic PrinciplesDokumen1 halamanAyurvedic PrinciplesSanjay PisharodiBelum ada peringkat
- Dinacharya - AnswersDokumen7 halamanDinacharya - AnswersSanjay PisharodiBelum ada peringkat
- AH Last ClassDokumen1 halamanAH Last ClassSanjay PisharodiBelum ada peringkat
- Amavata Allowed Foods and RestrictionsDokumen1 halamanAmavata Allowed Foods and RestrictionsSanjay PisharodiBelum ada peringkat
- Proposal For Goverdhan EcoDokumen3 halamanProposal For Goverdhan EcoSanjay PisharodiBelum ada peringkat
- Class by DR Sasikumar SirDokumen5 halamanClass by DR Sasikumar SirSanjay PisharodiBelum ada peringkat
- Panchakarma AnswersDokumen1 halamanPanchakarma AnswersSanjay PisharodiBelum ada peringkat
- SexualityDokumen2 halamanSexualitySanjay Pisharodi100% (1)
- VatashonitaDokumen1 halamanVatashonitaSanjay PisharodiBelum ada peringkat
- DR Susheela SeminarDokumen1 halamanDR Susheela SeminarSanjay PisharodiBelum ada peringkat
- Ayurvedic Case SheetDokumen2 halamanAyurvedic Case SheetSanjay Pisharodi100% (4)
- Sexuality in AstrologyDokumen1 halamanSexuality in AstrologySanjay PisharodiBelum ada peringkat
- Ayurveda For MenDokumen2 halamanAyurveda For MenSanjay PisharodiBelum ada peringkat
- CoverDokumen1 halamanCoverSanjay PisharodiBelum ada peringkat
- History - MajjandaDokumen1 halamanHistory - MajjandaSanjay PisharodiBelum ada peringkat
- Purnarogya PamphletDokumen2 halamanPurnarogya PamphletSanjay PisharodiBelum ada peringkat
- DAMA FormDokumen1 halamanDAMA FormSanjay PisharodiBelum ada peringkat
- Statement of CreditDokumen1 halamanStatement of CreditSanjay PisharodiBelum ada peringkat
- Supplement-2 - DR SanjayDokumen2 halamanSupplement-2 - DR SanjaySanjay PisharodiBelum ada peringkat
- Clinical Efficacy of Eranda Muladi Yapana Basti in The Management of Kati Graha (Lumbar Spondylosis)Dokumen21 halamanClinical Efficacy of Eranda Muladi Yapana Basti in The Management of Kati Graha (Lumbar Spondylosis)Sanjay PisharodiBelum ada peringkat
- Free Consultation: Ayurvedic Tradition, Right Here in Vrindavan. Guided by ADokumen3 halamanFree Consultation: Ayurvedic Tradition, Right Here in Vrindavan. Guided by ASanjay PisharodiBelum ada peringkat
- Agnihotra MantrasDokumen2 halamanAgnihotra MantrasSanjay PisharodiBelum ada peringkat
- Document 1 Education DisclosureDokumen1 halamanDocument 1 Education DisclosureSanjay PisharodiBelum ada peringkat
- Provider ApplicationDokumen3 halamanProvider ApplicationSanjay PisharodiBelum ada peringkat
- Ayurvedic Case SheetDokumen2 halamanAyurvedic Case SheetSanjay Pisharodi100% (4)
- Patient Examination in AyurvedaDokumen2 halamanPatient Examination in AyurvedaSanjay PisharodiBelum ada peringkat
- Avarana 1Dokumen4 halamanAvarana 1Sanjay PisharodiBelum ada peringkat
- Purna Rog Ya 108Dokumen1 halamanPurna Rog Ya 108Sanjay PisharodiBelum ada peringkat
- CCRAS Books by PostDokumen5 halamanCCRAS Books by PostSanjay PisharodiBelum ada peringkat
- C 39Dokumen8 halamanC 39Tammie Gore100% (2)
- Urinary Tract Infections (UTIs): Causes, Symptoms & TreatmentDokumen22 halamanUrinary Tract Infections (UTIs): Causes, Symptoms & TreatmentNoor AliBelum ada peringkat
- Physiology of The KidneysDokumen8 halamanPhysiology of The Kidneysor1da2sa3Belum ada peringkat
- CRNE Nursing Prioritization, Isolation, Infection ClassificationDokumen10 halamanCRNE Nursing Prioritization, Isolation, Infection ClassificationBreanne Corbeels100% (4)
- Ayurvedic plant profile of Crataeva religiosa for kidney stonesDokumen7 halamanAyurvedic plant profile of Crataeva religiosa for kidney stonesudaysing patilBelum ada peringkat
- L 3 The Urinary Bladder& UrethraDokumen28 halamanL 3 The Urinary Bladder& UrethraAdnan Al-aniBelum ada peringkat
- Nbns2203 Renal and Endocrine NursingDokumen10 halamanNbns2203 Renal and Endocrine Nursingdicky chongBelum ada peringkat
- Microprotein Xsys0027 DDokumen4 halamanMicroprotein Xsys0027 DRajkishor YadavBelum ada peringkat
- Aubf Answer Key AubfDokumen56 halamanAubf Answer Key AubfFenyl Isis GuigayomaBelum ada peringkat
- Zoo 1 Excretion and OsmoregulationDokumen17 halamanZoo 1 Excretion and OsmoregulationMaheshkumar KalalBelum ada peringkat
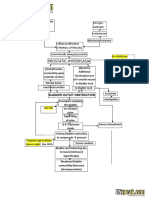
- Benign Prostatic Hyperplasia BPH Pathophysiology Schematic Diagram PDFDokumen2 halamanBenign Prostatic Hyperplasia BPH Pathophysiology Schematic Diagram PDFgailBelum ada peringkat
- L-9 The Excretory System: A. Multiple Choice TypeDokumen6 halamanL-9 The Excretory System: A. Multiple Choice TypeNeha ChandelBelum ada peringkat
- Dr. Dwi Rita Anggraini, M.Kes Dr. Sufitni, M.Kes Anatomy Department Medicine Faculty of North SumatraDokumen19 halamanDr. Dwi Rita Anggraini, M.Kes Dr. Sufitni, M.Kes Anatomy Department Medicine Faculty of North SumatraAnnDianaJaiminBelum ada peringkat
- EnuresisDokumen94 halamanEnuresisLucia ArdeleanBelum ada peringkat
- Water Needs and Hydration for PetsDokumen9 halamanWater Needs and Hydration for Petsann nnBelum ada peringkat
- Female CatheterizationDokumen64 halamanFemale CatheterizationLara Marie MACALINTALBelum ada peringkat
- Waste Management Techncial Brief Ochmo 021020Dokumen13 halamanWaste Management Techncial Brief Ochmo 021020Mohammad KhasawnehBelum ada peringkat
- Investigations of The Urinary TractDokumen26 halamanInvestigations of The Urinary TractOnkar SinghBelum ada peringkat
- Urinary SystemDokumen5 halamanUrinary SystemDonnabell DayudayBelum ada peringkat
- Urology Procedure and Diagnosis RatesDokumen10 halamanUrology Procedure and Diagnosis RatesNandarBelum ada peringkat
- Excretory Product and Their Elimination - Short Notes - Arjuna NEET 2024Dokumen4 halamanExcretory Product and Their Elimination - Short Notes - Arjuna NEET 2024TANISHQ JAINBelum ada peringkat
- Urinary System ReportDokumen8 halamanUrinary System ReportZilocke Gelera AmerilaBelum ada peringkat
- Urinary Tract Infections (UTI)Dokumen32 halamanUrinary Tract Infections (UTI)Ruqaya HassanBelum ada peringkat
- Wix212 en V1.0 Ifu Ce-MdrDokumen24 halamanWix212 en V1.0 Ifu Ce-MdrRaydoon SadeqBelum ada peringkat
- 03 Life Processes Chapter Wise Important QuestionsDokumen17 halaman03 Life Processes Chapter Wise Important Questionsmm8871100% (1)
- Vanguardia's Online Review Program: Genito-Urinary Tract FunctionDokumen8 halamanVanguardia's Online Review Program: Genito-Urinary Tract FunctionBobet ReñaBelum ada peringkat
- VBA-21-0960J-4-ARE Urinary PDFDokumen4 halamanVBA-21-0960J-4-ARE Urinary PDFCombat CraigBelum ada peringkat
- Bio MCQ TestDokumen23 halamanBio MCQ TestMalay ParikhBelum ada peringkat