Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Hiv Aids: Ika Norcahyanti Farmasi Klinik & Komunitas Fakultas Farmasi UNEJDokumen45 halamanHiv Aids: Ika Norcahyanti Farmasi Klinik & Komunitas Fakultas Farmasi UNEJMia RiswaniBelum ada peringkat
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- ParameterDokumen2 halamanParameterMia RiswaniBelum ada peringkat
- FtirDokumen4 halamanFtirMia RiswaniBelum ada peringkat
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Pelepasan Dan Penetrasi Natrium Diklofenak Sistem Niosom Span 60 Dalam Basis Gel HPMC 4000Dokumen12 halamanPelepasan Dan Penetrasi Natrium Diklofenak Sistem Niosom Span 60 Dalam Basis Gel HPMC 4000Mia RiswaniBelum ada peringkat
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Standar Neonatal Parenteral NutritionDokumen11 halamanStandar Neonatal Parenteral NutritionSitaBelum ada peringkat
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Aci Parenteral Nutrition PBDokumen72 halamanAci Parenteral Nutrition PBinkpen56789Belum ada peringkat
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Jadwal Praktikum Biofarmasetika New PDFDokumen6 halamanJadwal Praktikum Biofarmasetika New PDFMia RiswaniBelum ada peringkat
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Sediaan Steril (Compatibility Mode)Dokumen48 halamanSediaan Steril (Compatibility Mode)Yusup Dadan SaoriBelum ada peringkat
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Materials and MethodsDokumen4 halamanMaterials and MethodsMia RiswaniBelum ada peringkat
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- Traditional Medicinal Plants Used For The Treatment of Diabetes in Rural and Urban Areas of Dhaka, Bangladesh - An Ethnobotanical SurveyDokumen8 halamanTraditional Medicinal Plants Used For The Treatment of Diabetes in Rural and Urban Areas of Dhaka, Bangladesh - An Ethnobotanical SurveyMia RiswaniBelum ada peringkat
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
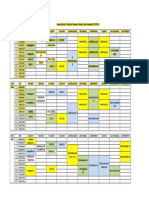
- Jadwal Kuliah & Praktikum Semester Genap Tahun Akademik 2013/2014Dokumen2 halamanJadwal Kuliah & Praktikum Semester Genap Tahun Akademik 2013/2014Mia RiswaniBelum ada peringkat
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- 2014 878646Dokumen3 halaman2014 878646Mia RiswaniBelum ada peringkat
- Jurnal 3 LihatDokumen10 halamanJurnal 3 LihatMia RiswaniBelum ada peringkat
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- 256 559 1 PB PDFDokumen12 halaman256 559 1 PB PDFMia RiswaniBelum ada peringkat
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- 256 559 1 PB PDFDokumen12 halaman256 559 1 PB PDFMia RiswaniBelum ada peringkat
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Free Electron TheoryDokumen8 halamanFree Electron TheoryNeelam KapoorBelum ada peringkat
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Entero SequencesDokumen12 halamanEntero SequencesKelvin SueyzyBelum ada peringkat
- Asco Series 238 ASCO Pilot Operated Solenoid Valves (Floating Diaphragm)Dokumen2 halamanAsco Series 238 ASCO Pilot Operated Solenoid Valves (Floating Diaphragm)Khyle Laurenz DuroBelum ada peringkat
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- SMC VM Eu PDFDokumen66 halamanSMC VM Eu PDFjoguvBelum ada peringkat
- Coffee Quality Manual by Abra Rand Nig Use IDokumen25 halamanCoffee Quality Manual by Abra Rand Nig Use IIpungBelum ada peringkat
- BITS Pilani: Determination of Extreme Pressure, Wear Preventive Characteristics of Lubricants Using Four Ball TesterDokumen10 halamanBITS Pilani: Determination of Extreme Pressure, Wear Preventive Characteristics of Lubricants Using Four Ball Testerakash chBelum ada peringkat
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Usp Description and SolubilityDokumen1 halamanUsp Description and SolubilityvafaashkBelum ada peringkat
- Psle Science Keywords !Dokumen12 halamanPsle Science Keywords !Aftertea CarousellBelum ada peringkat
- Đề 17Dokumen11 halamanĐề 17Nguyen CuongBelum ada peringkat
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Karl MarxDokumen4 halamanKarl Marxeirvine noah isidroBelum ada peringkat
- Medical GeneticsDokumen4 halamanMedical GeneticsCpopBelum ada peringkat
- Adriano Costa Sampaio: Electrical EngineerDokumen3 halamanAdriano Costa Sampaio: Electrical EngineeradrianorexBelum ada peringkat
- Book Index The Art of Heavy TransportDokumen6 halamanBook Index The Art of Heavy TransportHermon Pakpahan50% (2)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (120)
- Conquest CXAX Air-to-Water Heat PumpDokumen6 halamanConquest CXAX Air-to-Water Heat PumpAlexandre LopesBelum ada peringkat
- Raneem AlbazazDokumen33 halamanRaneem AlbazazGordana PuzovicBelum ada peringkat
- Veronte Autopilot Kit DatasheetDokumen2 halamanVeronte Autopilot Kit DatasheetEkmedzicBelum ada peringkat
- Chapter 7: Protein Function Part I: Myoglobin and HemoglobinDokumen27 halamanChapter 7: Protein Function Part I: Myoglobin and HemoglobineliBelum ada peringkat
- Indoor Air Quality Standard Procedures - 2014 RevDokumen12 halamanIndoor Air Quality Standard Procedures - 2014 RevFioriAmeliaHathawayBelum ada peringkat
- Wang Jinhui - Competitive Physics - Thermodynamics, Electromagnetism and Relativity (2019, World Scientific Publishing Co. Pte. LTD.)Dokumen961 halamanWang Jinhui - Competitive Physics - Thermodynamics, Electromagnetism and Relativity (2019, World Scientific Publishing Co. Pte. LTD.)Paritosh PandeyBelum ada peringkat
- Flow Zone Indicator Guided Workflows For PetrelDokumen11 halamanFlow Zone Indicator Guided Workflows For PetrelAiwarikiaar100% (1)
- Comparative Study On Serial and Parallel Manipulators - ReviewDokumen23 halamanComparative Study On Serial and Parallel Manipulators - ReviewShaik Himam SahebBelum ada peringkat
- Carrefour-SA Shopping Center TurkeyDokumen2 halamanCarrefour-SA Shopping Center TurkeyVineet JogalekarBelum ada peringkat
- ContempoDokumen4 halamanContempoPrincess Jonette YumulBelum ada peringkat
- Optical Scattering of Gold NanosphereDokumen24 halamanOptical Scattering of Gold NanosphereParas KumarBelum ada peringkat
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Eco Exercise 3answer Ans 1Dokumen8 halamanEco Exercise 3answer Ans 1Glory PrintingBelum ada peringkat
- Investigation of Skew Curved Bridges in Combination With Skewed Abutments Under Seismic ResponseDokumen5 halamanInvestigation of Skew Curved Bridges in Combination With Skewed Abutments Under Seismic ResponseEditor IJTSRDBelum ada peringkat
- Javanese PeopleDokumen22 halamanJavanese PeopleDenisaBelum ada peringkat
- Manual of Sensorless Brushless Motor Speed Controller: Pentium SeriesDokumen4 halamanManual of Sensorless Brushless Motor Speed Controller: Pentium Seriesfosavo5839Belum ada peringkat
- Kelas ChondrichtyesDokumen15 halamanKelas ChondrichtyesanitagustinawatiBelum ada peringkat
- Smart Grid TechnologyDokumen43 halamanSmart Grid Technologyarnav LakshkarBelum ada peringkat
- Organic Chemistry for Schools: Advanced Level and Senior High SchoolDari EverandOrganic Chemistry for Schools: Advanced Level and Senior High SchoolBelum ada peringkat
- Periodic Tales: A Cultural History of the Elements, from Arsenic to ZincDari EverandPeriodic Tales: A Cultural History of the Elements, from Arsenic to ZincPenilaian: 3.5 dari 5 bintang3.5/5 (137)