Anda mungkin juga menyukai
- Common Cutaneous Disorders in ElderlyDokumen6 halamanCommon Cutaneous Disorders in Elderlyirvinaldi9Belum ada peringkat
- Bercak MerahDokumen16 halamanBercak MerahFary SatriadiBelum ada peringkat
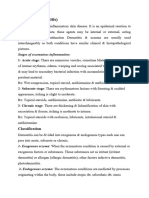
- Acute Inflammatory DermatosesDokumen29 halamanAcute Inflammatory DermatosesHaniya KhanBelum ada peringkat
- Hand DermatitisDokumen6 halamanHand Dermatitisminerva_stanciuBelum ada peringkat
- Contact DermatitisDokumen4 halamanContact DermatitisErlangga D SaputroBelum ada peringkat
- Complete Medical Guide for Disease Volume VII; Atopic DermatitisDari EverandComplete Medical Guide for Disease Volume VII; Atopic DermatitisBelum ada peringkat
- Irritant Contact DermatitisDokumen13 halamanIrritant Contact DermatitisYoga Alfian NoorBelum ada peringkat
- Asuhan Keperawatan Gangguan Sistem Integumentum Pada LansiaDokumen50 halamanAsuhan Keperawatan Gangguan Sistem Integumentum Pada LansiadwiinasBelum ada peringkat
- ECZEMADokumen4 halamanECZEMAAMOS MELIBelum ada peringkat
- Successful Control of Some Challenging Cases in Late Adult and Elderly Onset Atopic Dermatitis With Dupilumab Injection in Kuwaiti Patients A Prospective Pilot StudyDokumen10 halamanSuccessful Control of Some Challenging Cases in Late Adult and Elderly Onset Atopic Dermatitis With Dupilumab Injection in Kuwaiti Patients A Prospective Pilot StudyAthenaeum Scientific PublishersBelum ada peringkat
- Contact Dermatitis in ChildrenDokumen6 halamanContact Dermatitis in ChildrenYogi SanjayaBelum ada peringkat
- Dermatitis Numularis and NeurodermatitisDokumen22 halamanDermatitis Numularis and NeurodermatitisNura ReefaBelum ada peringkat
- PDF DocumentDokumen4 halamanPDF DocumentAditya Yudha PratamaBelum ada peringkat
- Toxic Responses of The SkinDokumen25 halamanToxic Responses of The SkinfianceeleeBelum ada peringkat
- Emedicine Lapkas 2Dokumen12 halamanEmedicine Lapkas 2Althaf FathanBelum ada peringkat
- Dermatitis Numularis PDFDokumen3 halamanDermatitis Numularis PDFRiska Permata SariBelum ada peringkat
- Red EyesDokumen3 halamanRed EyesirijoaBelum ada peringkat
- University of Hargeisa Facualt of Applied ScienceDokumen5 halamanUniversity of Hargeisa Facualt of Applied ScienceAwdahir JuniorBelum ada peringkat
- محاضرة 4Dokumen7 halamanمحاضرة 4rahaf.almomaniBelum ada peringkat
- Anaesthesia - May 1984 - SMITH - Anaesthesia and Severe Skin DiseaseDokumen13 halamanAnaesthesia - May 1984 - SMITH - Anaesthesia and Severe Skin DiseaseSaad AslamBelum ada peringkat
- Atopic Dermatitis: From Pathophysiology To Diagnostic ApproachDokumen9 halamanAtopic Dermatitis: From Pathophysiology To Diagnostic Approachwe sagara dewiBelum ada peringkat
- 2 EczemaDokumen5 halaman2 Eczemaحسين طاهر حاتم طاهرBelum ada peringkat
- Cap. 10. SKIN DISEASES PDFDokumen14 halamanCap. 10. SKIN DISEASES PDFoana policarpovBelum ada peringkat
- Patho-Physiology Pharm Lecture 11Dokumen15 halamanPatho-Physiology Pharm Lecture 11Manar AlzobiBelum ada peringkat
- Epidemiology of Skin DiseasesDokumen33 halamanEpidemiology of Skin DiseasesMahmoud AbuAwadBelum ada peringkat
- Presentation PhytoDokumen57 halamanPresentation Phytoyasmeenelraouf16Belum ada peringkat
- Dermato - Emergemencies (Acute Blistering and Exfoliative Skin) Nyoman Suryawati ObjectiveDokumen9 halamanDermato - Emergemencies (Acute Blistering and Exfoliative Skin) Nyoman Suryawati ObjectiveLong LieBelum ada peringkat
- Contact Dermatitis: Key PointsDokumen8 halamanContact Dermatitis: Key Pointssaimon reyBelum ada peringkat
- 002 - Additional MaterialDokumen30 halaman002 - Additional MaterialLucas Victor AlmeidaBelum ada peringkat
- DermatitisDokumen46 halamanDermatitisHadi AbdulhadiBelum ada peringkat
- Irritant Contact DermatitisDokumen5 halamanIrritant Contact DermatitisJohn P M SinagaBelum ada peringkat
- ErythrodermaDokumen48 halamanErythrodermaShwan OmarBelum ada peringkat
- Staphylococcus, Seasonal Variation, Alcohol and Drugs. The Allergens CommonlyDokumen3 halamanStaphylococcus, Seasonal Variation, Alcohol and Drugs. The Allergens CommonlyImam DermawanBelum ada peringkat
- Allergic Contact DermatitisDokumen11 halamanAllergic Contact DermatitisSf AkhadiyatiBelum ada peringkat
- CCJM Distinguishing Cellulitis From Its MimicsDokumen6 halamanCCJM Distinguishing Cellulitis From Its MimicsBrian HarrisBelum ada peringkat
- Laporan Pendahuluan DermatitisDokumen18 halamanLaporan Pendahuluan DermatitisIRGZI AULIAHAQBelum ada peringkat
- Cap 16 Schwatz - Pyoderma Gangrenosum (PG) : SummaryDokumen2 halamanCap 16 Schwatz - Pyoderma Gangrenosum (PG) : SummaryLuca VaccaroBelum ada peringkat
- Atopic Dermatitis & MelanomaDokumen15 halamanAtopic Dermatitis & MelanomaShalu RjBelum ada peringkat
- Icthyosis As A Manifestation of Internal DiseaseDokumen24 halamanIcthyosis As A Manifestation of Internal DiseaseSRIRAM CKBelum ada peringkat
- Penyakit Dermatitis: Dr. Kristo A. Nababan, SPKKDokumen47 halamanPenyakit Dermatitis: Dr. Kristo A. Nababan, SPKKDaniel Suarez ParapatBelum ada peringkat
- Scientific Revolution in Ayurveda!: Dyshidrotic Eczema: A PerspectiveDokumen7 halamanScientific Revolution in Ayurveda!: Dyshidrotic Eczema: A PerspectiveDwitiara SeptianiBelum ada peringkat
- Kostner 2017Dokumen12 halamanKostner 2017Daisy HamdaliBelum ada peringkat
- Kuliah SMTR VDokumen117 halamanKuliah SMTR VHorakhty PrideBelum ada peringkat
- Dermatitis and Eczema: Ailing Zou (邹爱玲) 2021.10.18Dokumen31 halamanDermatitis and Eczema: Ailing Zou (邹爱玲) 2021.10.18AmeliaBelum ada peringkat
- Dermatitides, Eczema, NeurodermatoseDokumen20 halamanDermatitides, Eczema, NeurodermatoseElephant ksmileBelum ada peringkat
- EczemapaperDokumen2 halamanEczemapaperapi-313697549Belum ada peringkat
- Dermatitis DR Citra 260907Dokumen56 halamanDermatitis DR Citra 260907Adam AriwibawaBelum ada peringkat
- Permasalahan Kulit Pada UsilaDokumen31 halamanPermasalahan Kulit Pada UsilaetylienBelum ada peringkat
- Exfoliative DermatitisDokumen7 halamanExfoliative DermatitisRidyah Ning TyasBelum ada peringkat
- Inflammatory Skin DiseaseDokumen32 halamanInflammatory Skin Diseaseragnarok meroBelum ada peringkat
- Dermatitis & Urticaria: Department of Dermato Venereology Faculty of Medicine Gadjah Mada UniversityDokumen34 halamanDermatitis & Urticaria: Department of Dermato Venereology Faculty of Medicine Gadjah Mada UniversityadystiBelum ada peringkat
- Disorders of Abnormal KeratinizationDokumen36 halamanDisorders of Abnormal KeratinizationdayangBelum ada peringkat
- Skin Disease and Old Age: Key PointsDokumen9 halamanSkin Disease and Old Age: Key PointsAli HadjinBelum ada peringkat
- Eczema in Elderly PeopleDokumen1 halamanEczema in Elderly Peoplerwatson2208Belum ada peringkat
- Oral Versus Parenteral TherapyDokumen7 halamanOral Versus Parenteral TherapymanuelBelum ada peringkat
- Pathology of Integument System: Djoko Legowo, Mkes., DRHDokumen135 halamanPathology of Integument System: Djoko Legowo, Mkes., DRHPilar Mitra QurbanBelum ada peringkat
- Bacterial and Viral Infection in DermatologyDokumen33 halamanBacterial and Viral Infection in DermatologySeniwatyismailBelum ada peringkat
- Assalamu'alikum WR WB: Harijono KariosentonoDokumen59 halamanAssalamu'alikum WR WB: Harijono KariosentonoDhiastikaBelum ada peringkat
- Atopic Dermatitis PresentsiDokumen17 halamanAtopic Dermatitis PresentsianniBelum ada peringkat
- Medical Journals Year in Body Mods 2012 12-30-12Dokumen24 halamanMedical Journals Year in Body Mods 2012 12-30-12Hadi FirmansyahBelum ada peringkat
- Fatal Metastatic Cutaneous Squamous Cell Carcinoma Evolving From A Localized Verrucous Epidermal NevusDokumen11 halamanFatal Metastatic Cutaneous Squamous Cell Carcinoma Evolving From A Localized Verrucous Epidermal NevusHadi FirmansyahBelum ada peringkat
- Lower Blepharoplasty: How To Avoid Complications: Dr. Vincent KH KWANDokumen3 halamanLower Blepharoplasty: How To Avoid Complications: Dr. Vincent KH KWANHadi FirmansyahBelum ada peringkat
- Collodion Baby and Loricrin Keratoderma: A Case Report and Mutation AnalysisDokumen5 halamanCollodion Baby and Loricrin Keratoderma: A Case Report and Mutation AnalysisHadi FirmansyahBelum ada peringkat
- Cutaneous Annular Sarcoidosis Developing On A Background of Exogenous Ochronosis: A Report of Two Cases and Review of The LiteratureDokumen5 halamanCutaneous Annular Sarcoidosis Developing On A Background of Exogenous Ochronosis: A Report of Two Cases and Review of The LiteratureHadi FirmansyahBelum ada peringkat
- Dermatologica Sinica: Cheng-Han Lee, Yi-Chun Chen, Yung-Tsu Cho, Chia-Ying Chang, Chia-Yu ChuDokumen5 halamanDermatologica Sinica: Cheng-Han Lee, Yi-Chun Chen, Yung-Tsu Cho, Chia-Ying Chang, Chia-Yu ChuHadi FirmansyahBelum ada peringkat
- New Developments in Ochronosis: Review of The LiteratureDokumen6 halamanNew Developments in Ochronosis: Review of The LiteratureHadi FirmansyahBelum ada peringkat
- Thayer Martin Agar Procedure 08Dokumen1 halamanThayer Martin Agar Procedure 08Hadi FirmansyahBelum ada peringkat
- Jurnal AlergiDokumen6 halamanJurnal AlergiHadi FirmansyahBelum ada peringkat
- Jcad 6 8 23Dokumen6 halamanJcad 6 8 23Hadi FirmansyahBelum ada peringkat
- Salient Features of The National Health Policy - 2017: July 2019Dokumen3 halamanSalient Features of The National Health Policy - 2017: July 2019Deepanshu JharkhandeBelum ada peringkat
- Long Term Follow Up After Admin Human GT Products - Jan - 2020Dokumen37 halamanLong Term Follow Up After Admin Human GT Products - Jan - 2020DBelum ada peringkat
- Sociology PresentationDokumen31 halamanSociology PresentationNirbhay SinghBelum ada peringkat
- Your Body Believes Every Word Y - Barbara Hoberman LevineDokumen380 halamanYour Body Believes Every Word Y - Barbara Hoberman LevineRoryBradshawBelum ada peringkat
- A2 - Practice 29Dokumen2 halamanA2 - Practice 29123VinhcuuBelum ada peringkat
- Prognostic Factors and Management of Patients With Choanal AtresiaDokumen7 halamanPrognostic Factors and Management of Patients With Choanal Atresiafarah maulida martaBelum ada peringkat
- Natural Medicine IODINE by Sue Visser.4810627Dokumen3 halamanNatural Medicine IODINE by Sue Visser.4810627relativelabs2075Belum ada peringkat
- List COVID Facilities State OdishaDokumen3 halamanList COVID Facilities State OdishadrjyotivetBelum ada peringkat
- Shingles (Herpes Zoster)Dokumen5 halamanShingles (Herpes Zoster)ceciliafanyBelum ada peringkat
- A Simple Approach To Shared Decision Making in Cancer ScreeningDokumen6 halamanA Simple Approach To Shared Decision Making in Cancer ScreeningariskaBelum ada peringkat
- 100 Test Aarogya 2.0:: Mrs - Gunjan MisraDokumen19 halaman100 Test Aarogya 2.0:: Mrs - Gunjan Misramomo misraBelum ada peringkat
- English Grade 4. Unit 6 Healthy World LP 3Dokumen3 halamanEnglish Grade 4. Unit 6 Healthy World LP 3Акниет РахметоваBelum ada peringkat
- Risk Factors For CKDDokumen2 halamanRisk Factors For CKDgigolo13Belum ada peringkat
- Floppy BabyDokumen13 halamanFloppy BabyJorge JhgBelum ada peringkat
- Amniotic MembraneDokumen8 halamanAmniotic Membraneapi-481789048Belum ada peringkat
- Guideline Who Preeclampsia-EclampsiaDokumen48 halamanGuideline Who Preeclampsia-EclampsiaRahmania Noor AdibaBelum ada peringkat
- Comparative Study of Ashwatha Ksheer Sutra and Udumber Ksheer Sutra in The Management of Bhagandara (Fistula in ANO)Dokumen9 halamanComparative Study of Ashwatha Ksheer Sutra and Udumber Ksheer Sutra in The Management of Bhagandara (Fistula in ANO)International Journal of Innovative Science and Research TechnologyBelum ada peringkat
- Hidetaka Nomura Et Al. (2015)Dokumen4 halamanHidetaka Nomura Et Al. (2015)Janardana GedeBelum ada peringkat
- Đề Thi Học Kì 1 - Lớp 10Dokumen10 halamanĐề Thi Học Kì 1 - Lớp 10Châu HoàngBelum ada peringkat
- The Sixth House - Psychology of Self-Integration - Robert Glasscock - B00F07KNZ0 - EBOKDokumen155 halamanThe Sixth House - Psychology of Self-Integration - Robert Glasscock - B00F07KNZ0 - EBOKAndrew Khabaza100% (6)
- General Biology Reviewer (2: I. PLANT BIOLOGY: Anatomy and PhysiologyDokumen12 halamanGeneral Biology Reviewer (2: I. PLANT BIOLOGY: Anatomy and Physiologymarie parfanBelum ada peringkat
- Homeostasis Case StudyDokumen3 halamanHomeostasis Case Studyapi-332887331Belum ada peringkat
- Cross Taping - A Practical Guide 12Dokumen2 halamanCross Taping - A Practical Guide 12jfjjfjfjjfjfBelum ada peringkat
- Wolf PresentationDokumen35 halamanWolf PresentationTahir Bin AbdullahBelum ada peringkat
- PDFDokumen732 halamanPDFMahmud Eljaarani90% (10)
- Nutritional Prehabilitation Program and Cardiac Surgery Outcome in PediatricsDokumen15 halamanNutritional Prehabilitation Program and Cardiac Surgery Outcome in PediatricsIOSRjournalBelum ada peringkat
- Lapsus Dr. DodyDokumen36 halamanLapsus Dr. DodyPriscilla Christina NatanBelum ada peringkat
- Class 12th Chemistry Project On Investigatory Test On GuavaDokumen20 halamanClass 12th Chemistry Project On Investigatory Test On GuavaAyush Kumar100% (1)
- Manual On Lab Referral For Outbreak Response-Draft 2Dokumen95 halamanManual On Lab Referral For Outbreak Response-Draft 2kbl27Belum ada peringkat
- Bowen NeglectDokumen46 halamanBowen NeglectwefwfwrBelum ada peringkat