Anda mungkin juga menyukai
- PT Consultation FormDokumen7 halamanPT Consultation FormRachelBelum ada peringkat
- Client Initial Assessment Worksheet: How Did You Here About Us or Who Referred You?Dokumen5 halamanClient Initial Assessment Worksheet: How Did You Here About Us or Who Referred You?api-335005776Belum ada peringkat
- Client Info FormDokumen2 halamanClient Info FormkamalsalmanBelum ada peringkat
- Physical Activity Readiness Questionnaire (PAR-Q) : Yes NoDokumen4 halamanPhysical Activity Readiness Questionnaire (PAR-Q) : Yes NoKaye JornadalBelum ada peringkat
- Health Questionnaire Form (HQF)Dokumen1 halamanHealth Questionnaire Form (HQF)salmanBelum ada peringkat
- Precision Nutrition Comprehensive Client Information Sheet PDFDokumen5 halamanPrecision Nutrition Comprehensive Client Information Sheet PDFJosh WarrellBelum ada peringkat
- Senior Exercise Resource GuideDokumen16 halamanSenior Exercise Resource GuideElham FarahmandBelum ada peringkat
- Registration BootcampDokumen8 halamanRegistration BootcampgreggniemannBelum ada peringkat
- Clearance For Safe Exercise Participation: I. Health HistoryDokumen3 halamanClearance For Safe Exercise Participation: I. Health HistoryejjohnsoBelum ada peringkat
- Informed Consent FormDokumen3 halamanInformed Consent Formapi-380169571Belum ada peringkat
- Personal Training Information PackageDokumen4 halamanPersonal Training Information PackageTalisman CentreBelum ada peringkat
- Personalized Exercise Program Questionnaire: Bangor YmcaDokumen4 halamanPersonalized Exercise Program Questionnaire: Bangor YmcaSusan MatayonBelum ada peringkat
- Assessment Done Prior To FitnessDokumen15 halamanAssessment Done Prior To FitnessAditya SharmaBelum ada peringkat
- Informed Consent AgreementDokumen2 halamanInformed Consent AgreementArbiarso WijatmokoBelum ada peringkat
- Knee Clinic Intake Forms 2013Dokumen4 halamanKnee Clinic Intake Forms 2013Dr. Dale MacdonaldBelum ada peringkat
- RFC 2 PAGE Physical 2010 With OnsetDokumen2 halamanRFC 2 PAGE Physical 2010 With OnsetghobbieBelum ada peringkat
- IMCOM Civilian Wellness Program PacketDokumen7 halamanIMCOM Civilian Wellness Program PacketU.S. Army's Family and Morale, Welfare and Recreation ProgramsBelum ada peringkat
- PT Consent Form PDFDokumen2 halamanPT Consent Form PDFPrashant Singh RajputBelum ada peringkat
- 2 - ParqDokumen4 halaman2 - Parqjsa.3512922Belum ada peringkat
- Clientintakeforms 1Dokumen17 halamanClientintakeforms 1api-256268960Belum ada peringkat
- Informed ConsentDokumen3 halamanInformed Consentapi-486168857Belum ada peringkat
- Diabetes QuestionnaireDokumen3 halamanDiabetes QuestionnaireHarishchowdary PemmasaniBelum ada peringkat
- Health Information PrintDokumen2 halamanHealth Information PrintCarole ArmsBelum ada peringkat
- Health Appraisal RecordDokumen2 halamanHealth Appraisal RecordRandy PacquiaoBelum ada peringkat
- CF 4820 Screening Rules Wavier 14 March 2015Dokumen7 halamanCF 4820 Screening Rules Wavier 14 March 2015api-138096780Belum ada peringkat
- MM SS Ankle FootDokumen3 halamanMM SS Ankle FootFernando100% (1)
- Jan Rydfors MD Facog, Rubi Khilnani MD FacogDokumen6 halamanJan Rydfors MD Facog, Rubi Khilnani MD FacogSantosh Kumar SinghBelum ada peringkat
- CITHMSG24 CITHM SPORTS CUP PARQ FormDokumen1 halamanCITHMSG24 CITHM SPORTS CUP PARQ Formpaoloramosramos0527Belum ada peringkat
- Personal Trainer FormsDokumen8 halamanPersonal Trainer FormsWes Geary100% (3)
- Health Appraisal Record: I. Personal Data: II. Physical and Medical ExaminationDokumen2 halamanHealth Appraisal Record: I. Personal Data: II. Physical and Medical ExaminationJA BerzabalBelum ada peringkat
- Urs Par QDokumen1 halamanUrs Par QDanielBelum ada peringkat
- CJ'S Functional Fitness Health Assessment FormDokumen3 halamanCJ'S Functional Fitness Health Assessment FormCleonJosephBelum ada peringkat
- Re-Examination/ Assessment of Improvement Name: - DateDokumen1 halamanRe-Examination/ Assessment of Improvement Name: - DatekaelielmtBelum ada peringkat
- AXE Medical Questionnaire and Informed ConsentDokumen1 halamanAXE Medical Questionnaire and Informed ConsentJefferson Kevin MorcoBelum ada peringkat
- Physical Activity Readiness Questionnaire (PAR-Q) : Yes NoDokumen4 halamanPhysical Activity Readiness Questionnaire (PAR-Q) : Yes NoDarren BernardoBelum ada peringkat
- Personal Training Health History QuestionaireDokumen4 halamanPersonal Training Health History QuestionaireJamie StaggBelum ada peringkat
- Informed Consent For Your Fitness AssessmentDokumen3 halamanInformed Consent For Your Fitness AssessmentWaldir Martins NetoBelum ada peringkat
- KHP Activity Class Par-QDokumen2 halamanKHP Activity Class Par-Qapi-741759851Belum ada peringkat
- Ealth Ertificate Ealth ErtificateDokumen1 halamanEalth Ertificate Ealth ErtificateRendra FelaniBelum ada peringkat
- Client Intake FormsDokumen5 halamanClient Intake FormsGuillaume VingtcentBelum ada peringkat
- New Health and HistoryDokumen3 halamanNew Health and HistorymredubzBelum ada peringkat
- 2020 Par-QDokumen2 halaman2020 Par-QMarilyn GalvoBelum ada peringkat
- PAR Q FormDokumen3 halamanPAR Q FormJaira Mier GalloBelum ada peringkat
- Learning Guide Physical Education 11 Grade 11-Abm/Humss/Stem SY: 2020-2021Dokumen12 halamanLearning Guide Physical Education 11 Grade 11-Abm/Humss/Stem SY: 2020-2021akaiaBelum ada peringkat
- Fitness Health Assessment FormDokumen4 halamanFitness Health Assessment FormTanmay DevBelum ada peringkat
- Personal Fitness MBDokumen14 halamanPersonal Fitness MBtom2susanBelum ada peringkat
- Massage Intake Form TemplateDokumen4 halamanMassage Intake Form TemplateronaBelum ada peringkat
- Client Assessment Form 2Dokumen2 halamanClient Assessment Form 2roshan karkiBelum ada peringkat
- Oil and Natural Gas Corporation LTD Self Declaration On Medical StatusDokumen4 halamanOil and Natural Gas Corporation LTD Self Declaration On Medical StatusDodiya NikunjBelum ada peringkat
- ChildparqwaiverDokumen1 halamanChildparqwaiverFilipe SilvérioBelum ada peringkat
- Bariatrics Weight Loss IntakeDokumen12 halamanBariatrics Weight Loss IntakeErin abelsBelum ada peringkat
- Basic Health Assessment - Screening and Consent FormDokumen2 halamanBasic Health Assessment - Screening and Consent FormjoshpollackBelum ada peringkat
- PAR Q FormDokumen3 halamanPAR Q FormZoila CamiasBelum ada peringkat
- Health Appraisal Record: I. Personal Data: II. Physical and Medical ExaminationDokumen2 halamanHealth Appraisal Record: I. Personal Data: II. Physical and Medical ExaminationJA BerzabalBelum ada peringkat
- Comprehensive Activity Program AishaDokumen13 halamanComprehensive Activity Program Aishaapi-569904702Belum ada peringkat
- 35b Employee TB Physical Form For Positive PPDDokumen1 halaman35b Employee TB Physical Form For Positive PPDkhaul508Belum ada peringkat
- HEALTH APPRAISAL RECORD SsDokumen3 halamanHEALTH APPRAISAL RECORD SsDaryl ZaldarriagaBelum ada peringkat
- PE and Health ModuleDokumen17 halamanPE and Health ModuleTessaKaye AlfaroBelum ada peringkat
- LAS1.2 - Week 2 - PEH11 - Physical Fitness TestDokumen11 halamanLAS1.2 - Week 2 - PEH11 - Physical Fitness TestMaricel EsperatBelum ada peringkat
- Baki Workout Program 2Dokumen7 halamanBaki Workout Program 2Plamen PetkovBelum ada peringkat
- Final Coaching For Class Tanglaw BlankDokumen23 halamanFinal Coaching For Class Tanglaw BlankFox GamingBelum ada peringkat
- AnimesDokumen4 halamanAnimeskosali4061Belum ada peringkat
- SIMD Machines:: Pipeline SystemDokumen35 halamanSIMD Machines:: Pipeline Systempssdk99hfdBelum ada peringkat
- Tennis Industry MagazineDokumen64 halamanTennis Industry MagazineLiya DavidovBelum ada peringkat
- 1 - Fair Grounds RetrospectosDokumen9 halaman1 - Fair Grounds Retrospectosjessy jamesBelum ada peringkat
- Esports: The World of Competitive Gaming: An OverviewDokumen19 halamanEsports: The World of Competitive Gaming: An OverviewYeison ChurquipaBelum ada peringkat
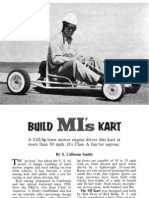
- Build Mechanics Illustrated KartDokumen7 halamanBuild Mechanics Illustrated KartJim100% (5)
- Speech For HIPDokumen2 halamanSpeech For HIPAbbyBelum ada peringkat
- Metric Handbook Planning AND Design Data: Edited by David AdlerDokumen13 halamanMetric Handbook Planning AND Design Data: Edited by David AdlerEng Venance Masanja100% (1)
- School Calendar 2008 2009Dokumen2 halamanSchool Calendar 2008 20094th Grade TeacherBelum ada peringkat
- Forensic Ballistics WK 3Dokumen18 halamanForensic Ballistics WK 3Jennielyn VillanuevaBelum ada peringkat
- Home Nano Volume 5 Additional List 6pp OnlyDokumen6 halamanHome Nano Volume 5 Additional List 6pp OnlyPaul Edgar GonzalesBelum ada peringkat
- Ip TVDokumen58 halamanIp TVArisBelum ada peringkat
- LithiumDokumen3 halamanLithiumTommaso ParmigianiBelum ada peringkat
- Cement - Mortar: Apparatus For Lime Testing Reactivity Air Content Meter 1 Litre CapacityDokumen1 halamanCement - Mortar: Apparatus For Lime Testing Reactivity Air Content Meter 1 Litre CapacityLESO IndustrialBelum ada peringkat
- Activity 4 - Having FunDokumen3 halamanActivity 4 - Having FunAndre Ortegon100% (1)
- Mob UaDokumen6 halamanMob Uasvaleev846fBelum ada peringkat
- 2010 BTYCatalogDokumen68 halaman2010 BTYCatalogceodossBelum ada peringkat
- Pajero Handbrake AdjustmentDokumen1 halamanPajero Handbrake AdjustmentNe TwentySixBelum ada peringkat
- BANSBACH Gas Springs Quick Ship Catalogue 2011enDokumen10 halamanBANSBACH Gas Springs Quick Ship Catalogue 2011enGustavo BermudezBelum ada peringkat
- List of Breath of Fire III AbilitiesDokumen22 halamanList of Breath of Fire III AbilitiesDuniesky Trujillo GarcíaBelum ada peringkat
- Training Camp 08 ProgramDokumen4 halamanTraining Camp 08 ProgramChetanya MundachaliBelum ada peringkat
- Read Carefully!: Official Rules and Regulations For MRSS Ka-Vroom Soapbox DerbyDokumen20 halamanRead Carefully!: Official Rules and Regulations For MRSS Ka-Vroom Soapbox DerbykavroomBelum ada peringkat
- Overtone Chart For Tenor and Bass TrombonesDokumen1 halamanOvertone Chart For Tenor and Bass Trombonesdenerin100% (1)
- CANFIT Training ProgramDokumen2 halamanCANFIT Training ProgramMatthew CittaBelum ada peringkat
- IdiomsDokumen3 halamanIdiomsGem MaBelum ada peringkat
- Mass DanceDokumen4 halamanMass DanceGHi YHanBelum ada peringkat
- Data Book: Automotive TechnicalDokumen1 halamanData Book: Automotive TechnicalW̶i̶l̶l̶i̶a̶m̶ Valer Yoi KoeBelum ada peringkat
- Power RankingsDokumen29 halamanPower RankingsFrydoom Brawl StarsBelum ada peringkat