Anda mungkin juga menyukai
- Basic Level of Dental Resins - Material Science & Technology: 4th Edition, 2nd VersionDari EverandBasic Level of Dental Resins - Material Science & Technology: 4th Edition, 2nd VersionBelum ada peringkat
- Lenin-Root Canal SealersDokumen117 halamanLenin-Root Canal SealersVidya SagarBelum ada peringkat
- 15.1 Root Canal SealersDokumen48 halaman15.1 Root Canal SealersRevathy M NairBelum ada peringkat
- Smear LayerDokumen114 halamanSmear LayerAME DENTAL COLLEGE RAICHUR, KARNATAKABelum ada peringkat
- JC 3Dokumen28 halamanJC 3achsah johnsonBelum ada peringkat
- Atypically Grown Large Periradicular Cyst Affecting Adjacent Teeth and Leading To Confounding Diagnosis of Non-Endodontic PathologyDokumen10 halamanAtypically Grown Large Periradicular Cyst Affecting Adjacent Teeth and Leading To Confounding Diagnosis of Non-Endodontic PathologyJorge OrbeBelum ada peringkat
- Calcium Hydroxide - Based Root Canal Sealers A Rewiew JENDODokumen6 halamanCalcium Hydroxide - Based Root Canal Sealers A Rewiew JENDODaniel Tavares TranninBelum ada peringkat
- Op Calcium HydroxideDokumen1 halamanOp Calcium HydroxideFaizal Prabowo KalimanBelum ada peringkat
- Basics of DOM FINALDokumen32 halamanBasics of DOM FINALachsah johnsonBelum ada peringkat
- Root Resorption Diagnosis, Classification and Treatment Choices Based On Stimulation FactorsDokumen8 halamanRoot Resorption Diagnosis, Classification and Treatment Choices Based On Stimulation FactorsAhmad AssariBelum ada peringkat
- Articulo de Crown DownDokumen13 halamanArticulo de Crown DownLaura DanielaBelum ada peringkat
- MTA-Based Root Canal Sealers PDFDokumen6 halamanMTA-Based Root Canal Sealers PDFAndrew GarciaBelum ada peringkat
- Present Status and Future Directions of Intracanal MedicamentsDokumen24 halamanPresent Status and Future Directions of Intracanal MedicamentsJavier VillalobosBelum ada peringkat
- Apical Seal Versus Coronal SealDokumen8 halamanApical Seal Versus Coronal SealSalem RawashdahBelum ada peringkat
- Clinical Research: SignificanceDokumen7 halamanClinical Research: SignificancejadeBelum ada peringkat
- Non Surgical Management of Periapical Lesions Using Calcium HydroxideDokumen6 halamanNon Surgical Management of Periapical Lesions Using Calcium HydroxideVinisha Vipin SharmaBelum ada peringkat
- "3Mix-MP in Endodontics - An Overview": Varalakshmi R Parasuraman MDS, Banker Sharadchandra Muljibhai MDSDokumen10 halaman"3Mix-MP in Endodontics - An Overview": Varalakshmi R Parasuraman MDS, Banker Sharadchandra Muljibhai MDSFirma Nurdinia DewiBelum ada peringkat
- EnamelDokumen9 halamanEnamelhustla7100% (1)
- Evaluation of Two Different Materials For Pre-Endodontic Restoration of Badly Destructed TeethDokumen7 halamanEvaluation of Two Different Materials For Pre-Endodontic Restoration of Badly Destructed TeethsrinandanBelum ada peringkat
- Pulp Dentin BiologyDokumen21 halamanPulp Dentin BiologyCristiane VazBelum ada peringkat
- Introduction To Dental MaterialsDokumen23 halamanIntroduction To Dental MaterialsAmar BimavarapuBelum ada peringkat
- Endodontic and Restorative Management of A Lower Molar With A Calcified Pulp Chamber.Dokumen7 halamanEndodontic and Restorative Management of A Lower Molar With A Calcified Pulp Chamber.Nicolas SantanderBelum ada peringkat
- Minimally Invasive When? How? Why?: Access Cavity Preparation in EndodonticsDokumen4 halamanMinimally Invasive When? How? Why?: Access Cavity Preparation in EndodonticsdoctorlupuBelum ada peringkat
- 17 Fracture MechanicsDokumen16 halaman17 Fracture MechanicsRevathy M NairBelum ada peringkat
- "Endodontic Sealers": Current Concepts and Comparative Analysis ReviewDokumen6 halaman"Endodontic Sealers": Current Concepts and Comparative Analysis ReviewAlina TomaBelum ada peringkat
- Antibiotic Medicaments ReviewDokumen10 halamanAntibiotic Medicaments ReviewGeorge ChackoBelum ada peringkat
- Dental CementDokumen12 halamanDental Cementshaniaz19785112Belum ada peringkat
- 10 1016@j Joen 2020 04 007Dokumen9 halaman10 1016@j Joen 2020 04 007rasagna reddyBelum ada peringkat
- Final Cases RassuDokumen35 halamanFinal Cases Rassurasagna reddyBelum ada peringkat
- 5 - Calcium Hydroxide Vs Mineral Trioxide Aggregates For Partial Pulpotomy of Permanent Molars With Deep Caries PDFDokumen6 halaman5 - Calcium Hydroxide Vs Mineral Trioxide Aggregates For Partial Pulpotomy of Permanent Molars With Deep Caries PDFAbdul Rahman AlmishhdanyBelum ada peringkat
- Kurtzman Restoration of Endodontically Treated TeethDokumen8 halamanKurtzman Restoration of Endodontically Treated TeethAdelia CaryabudiBelum ada peringkat
- Nanotechnology in Dentistry - Soon To Be Called NanodonticsDokumen12 halamanNanotechnology in Dentistry - Soon To Be Called NanodonticsIJAR JOURNAL100% (1)
- Pasta TripleDokumen7 halamanPasta TripleLincoln GarciaBelum ada peringkat
- Soumya S Jeena Profile BookDokumen53 halamanSoumya S Jeena Profile BooksoumyaBelum ada peringkat
- Universal Adhesives SlideDokumen73 halamanUniversal Adhesives SlidePawee PiyasowanBelum ada peringkat
- Splinting of Teeth Following TraumaDokumen73 halamanSplinting of Teeth Following TraumaSHRINIVAS GARJEBelum ada peringkat
- Endodontic Topics Volume 18 Issue 1 2008 (Doi 10.1111/j.1601-1546.2011.00260.x) YUAN-LING NG KISHOR GULABIVALA - Outcome of Non-Surgical Re-TreatmentDokumen28 halamanEndodontic Topics Volume 18 Issue 1 2008 (Doi 10.1111/j.1601-1546.2011.00260.x) YUAN-LING NG KISHOR GULABIVALA - Outcome of Non-Surgical Re-TreatmentardeleanoanaBelum ada peringkat
- Glass Ionomer Cement: Dept o EndodonticsDokumen67 halamanGlass Ionomer Cement: Dept o EndodonticsJayalakshmi Preetha100% (1)
- NazilaApplications of Nanotechnology in Endodontic - A ReviewDokumen6 halamanNazilaApplications of Nanotechnology in Endodontic - A ReviewElsa Di GiuseppeBelum ada peringkat
- C Shaped CanalDokumen24 halamanC Shaped CanalLo Chai LingBelum ada peringkat
- Intracanal MedicamentDokumen11 halamanIntracanal MedicamentAsh PeiBelum ada peringkat
- Minimally Invasive Dentistry 2Dokumen13 halamanMinimally Invasive Dentistry 2Asterix AsterixqueBelum ada peringkat
- Cleaning & Shaping of Root CANALS ..: Karishma Ashok Iv/Ii Roll No 31Dokumen24 halamanCleaning & Shaping of Root CANALS ..: Karishma Ashok Iv/Ii Roll No 31Poonam WavhalBelum ada peringkat
- EMI. Khademi, ClarkDokumen11 halamanEMI. Khademi, ClarkMaGe IsTeBelum ada peringkat
- Icdas Ii PDFDokumen30 halamanIcdas Ii PDFFarah ShazwanaBelum ada peringkat
- Principles in Esthetis DentistryDokumen82 halamanPrinciples in Esthetis DentistryMaria0% (1)
- Slide - 11 - Procedural AccidentsDokumen31 halamanSlide - 11 - Procedural AccidentsCWT2010100% (1)
- Prognosis of Initial Endodontic Therapy PDFDokumen30 halamanPrognosis of Initial Endodontic Therapy PDFRamona MateiBelum ada peringkat
- Apexification With MTADokumen9 halamanApexification With MTAIngrid PatriciaBelum ada peringkat
- Rely X PDFDokumen20 halamanRely X PDFSunita TipmontaBelum ada peringkat
- Intra Canal MedicamentsDokumen14 halamanIntra Canal MedicamentsS Noshin ShimiBelum ada peringkat
- Restoration of Endodontically Treated TeethDokumen17 halamanRestoration of Endodontically Treated TeethAfaf MagedBelum ada peringkat
- Pulp Capping MaterialDokumen21 halamanPulp Capping MaterialMohammad Abdul adheem100% (1)
- Obtaining Optimal Aesthetics With Veneered Zirconia and Lithium Disilicate Frameworks On Substrates of Different ColorsDokumen5 halamanObtaining Optimal Aesthetics With Veneered Zirconia and Lithium Disilicate Frameworks On Substrates of Different ColorsAna Maria Velez OchoaBelum ada peringkat
- Traumatic Injuries of The Tooth / Orthodontic Courses by Indian Dental AcademyDokumen43 halamanTraumatic Injuries of The Tooth / Orthodontic Courses by Indian Dental Academyindian dental academyBelum ada peringkat
- Nano-Antimicrobials in EndodonticsDokumen14 halamanNano-Antimicrobials in EndodonticsIJAR JOURNALBelum ada peringkat
- Recent Advances in DentistryDokumen2 halamanRecent Advances in DentistrySudarsan SangeethaBelum ada peringkat
- Obturation of The Root Canal System - Part I (Lecture by DR - Ahmed Labib @AmCoFam)Dokumen41 halamanObturation of The Root Canal System - Part I (Lecture by DR - Ahmed Labib @AmCoFam)AmericanCornerFamilyBelum ada peringkat
- 20220619150419root Canal Filling Materials Theme 16 17 64814 1Dokumen51 halaman20220619150419root Canal Filling Materials Theme 16 17 64814 1Crimsonine SacredTranquilBelum ada peringkat
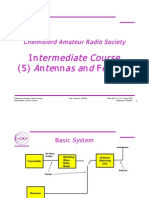
- Islide9 Antennas and FeedersDokumen14 halamanIslide9 Antennas and FeedersramchanderBelum ada peringkat
- Liquid Crystal Display Technology: Gregg CianfriniDokumen17 halamanLiquid Crystal Display Technology: Gregg CianfrinichadchoudBelum ada peringkat
- Liquid Crystal Display Technology: Gregg CianfriniDokumen17 halamanLiquid Crystal Display Technology: Gregg CianfrinichadchoudBelum ada peringkat
- Liquid Crystal Display Technology: Gregg CianfriniDokumen17 halamanLiquid Crystal Display Technology: Gregg CianfrinichadchoudBelum ada peringkat
- Liquid Crystal Display Technology: Gregg CianfriniDokumen17 halamanLiquid Crystal Display Technology: Gregg CianfrinichadchoudBelum ada peringkat
- Liquid Crystal Display Technology: Gregg CianfriniDokumen17 halamanLiquid Crystal Display Technology: Gregg CianfrinichadchoudBelum ada peringkat
- 1 Introduction To Sustainable Property Development: Sara J. Wilkinson and Sarah L. SayceDokumen64 halaman1 Introduction To Sustainable Property Development: Sara J. Wilkinson and Sarah L. Sayceb100% (1)
- Ms D Sarma Flex Adhesive 520 UkDokumen7 halamanMs D Sarma Flex Adhesive 520 UkDeepson JohnBelum ada peringkat
- Act 6+14Dokumen4 halamanAct 6+14min95Belum ada peringkat
- Unit 10 ReadingDokumen25 halamanUnit 10 ReadingKhánh An VũBelum ada peringkat
- Constant Head Permeability TestDokumen5 halamanConstant Head Permeability TestNAMBIRO EMMANUEL MULAYI100% (1)
- Typologies GSAS Design Assessment v2.1Dokumen180 halamanTypologies GSAS Design Assessment v2.1Dinesh GuptaBelum ada peringkat
- Ken Betwa ReportDokumen161 halamanKen Betwa ReportNazakat Hussain100% (1)
- DVI143 Neatpump EN 1209 PDFDokumen4 halamanDVI143 Neatpump EN 1209 PDFHamza BaraketBelum ada peringkat
- Idromar MC1J MC2J MC3J User Manual-CópiaDokumen42 halamanIdromar MC1J MC2J MC3J User Manual-CópiaRenato MagalhãesBelum ada peringkat
- A-Level-Chemistry Edexcel FACER Sample-Chapter PDFDokumen36 halamanA-Level-Chemistry Edexcel FACER Sample-Chapter PDFahamedBelum ada peringkat
- V30 PDFDokumen84 halamanV30 PDFLuis SiuLBelum ada peringkat
- ICPEP-3 AbstractDokumen146 halamanICPEP-3 Abstractisebmail100% (1)
- Loro SiphonicDokumen44 halamanLoro SiphonicdanateoBelum ada peringkat
- Magnisali, 2021Dokumen17 halamanMagnisali, 2021Milagros MontesBelum ada peringkat
- Group A Rawat Lab Presentation FinalDokumen96 halamanGroup A Rawat Lab Presentation Finalumair100% (3)
- Engineering Book-Chapter 1-6 DuluDokumen74 halamanEngineering Book-Chapter 1-6 DuluaryoBelum ada peringkat
- DC Water Seeks Input For Naming Tunnel Boring Machine: Press ReleaseDokumen3 halamanDC Water Seeks Input For Naming Tunnel Boring Machine: Press ReleaseScott RobertsBelum ada peringkat
- Study of Aeration Efficiency at WeirsDokumen10 halamanStudy of Aeration Efficiency at WeirsDiego Alejandro Sanchez FajardoBelum ada peringkat
- Module 1 - Basics of Soil Mechanics Finished (Compatibility Mode)Dokumen145 halamanModule 1 - Basics of Soil Mechanics Finished (Compatibility Mode)Sahil Jawa100% (1)
- Method Statement For Installation, Inspection & Testing & Commissioning of Plumbing & Sanitary and Storm Drainage SystemDokumen29 halamanMethod Statement For Installation, Inspection & Testing & Commissioning of Plumbing & Sanitary and Storm Drainage SystemmarvinBelum ada peringkat
- Marshall Et Al. (2020) Cyanide - PuyangoDokumen11 halamanMarshall Et Al. (2020) Cyanide - PuyangoMariela Huaripata HuaripataBelum ada peringkat
- SDS 037 Standard Winterclean EnglishDokumen9 halamanSDS 037 Standard Winterclean EnglishAnkitBelum ada peringkat
- Drawings List Phase 2Dokumen5 halamanDrawings List Phase 2Anil PuvadaBelum ada peringkat
- Ziqiu Feng - Literature Review Draft 1000-1500 Word DraftDokumen7 halamanZiqiu Feng - Literature Review Draft 1000-1500 Word Draftapi-586754027Belum ada peringkat
- Uniflair LeoDokumen84 halamanUniflair LeoanganBelum ada peringkat
- Farnsworth ProposalDokumen2 halamanFarnsworth ProposalJessica LangoneBelum ada peringkat
- Shop Fabricated Aboveground Tank Construction StandardsDokumen15 halamanShop Fabricated Aboveground Tank Construction StandardsadammzjinBelum ada peringkat
- Water: Engineering Chemistry-I Unit-6Dokumen70 halamanWater: Engineering Chemistry-I Unit-6Abhyudaya Rajput an idiotBelum ada peringkat
- DENAIR Direct Driven Air Compressor User Manual - EEI 2Dokumen34 halamanDENAIR Direct Driven Air Compressor User Manual - EEI 2Danny Chango75% (8)
- The Meura Mash Filter PDFDokumen7 halamanThe Meura Mash Filter PDFDumy Dumiterr0% (1)
- Sodium Bicarbonate: Nature's Unique First Aid RemedyDari EverandSodium Bicarbonate: Nature's Unique First Aid RemedyPenilaian: 5 dari 5 bintang5/5 (21)
- Process Plant Equipment: Operation, Control, and ReliabilityDari EverandProcess Plant Equipment: Operation, Control, and ReliabilityPenilaian: 5 dari 5 bintang5/5 (1)
- A New Approach to HAZOP of Complex Chemical ProcessesDari EverandA New Approach to HAZOP of Complex Chemical ProcessesBelum ada peringkat
- Guidelines for Chemical Process Quantitative Risk AnalysisDari EverandGuidelines for Chemical Process Quantitative Risk AnalysisPenilaian: 5 dari 5 bintang5/5 (1)
- Functional Safety from Scratch: A Practical Guide to Process Industry ApplicationsDari EverandFunctional Safety from Scratch: A Practical Guide to Process Industry ApplicationsBelum ada peringkat
- Physical and Chemical Equilibrium for Chemical EngineersDari EverandPhysical and Chemical Equilibrium for Chemical EngineersPenilaian: 5 dari 5 bintang5/5 (1)
- Phase Equilibria in Chemical EngineeringDari EverandPhase Equilibria in Chemical EngineeringPenilaian: 4 dari 5 bintang4/5 (11)
- Lees' Process Safety Essentials: Hazard Identification, Assessment and ControlDari EverandLees' Process Safety Essentials: Hazard Identification, Assessment and ControlPenilaian: 4 dari 5 bintang4/5 (4)
- Water-Based Paint Formulations, Vol. 3Dari EverandWater-Based Paint Formulations, Vol. 3Penilaian: 4.5 dari 5 bintang4.5/5 (6)
- Well Control for Completions and InterventionsDari EverandWell Control for Completions and InterventionsPenilaian: 4 dari 5 bintang4/5 (10)
- The HAZOP Leader's Handbook: How to Plan and Conduct Successful HAZOP StudiesDari EverandThe HAZOP Leader's Handbook: How to Plan and Conduct Successful HAZOP StudiesBelum ada peringkat
- Coupled CFD-DEM Modeling: Formulation, Implementation and Application to Multiphase FlowsDari EverandCoupled CFD-DEM Modeling: Formulation, Implementation and Application to Multiphase FlowsBelum ada peringkat
- High Pressure Phase Behaviour of Multicomponent Fluid MixturesDari EverandHigh Pressure Phase Behaviour of Multicomponent Fluid MixturesBelum ada peringkat
- Distillation Design and Control Using Aspen SimulationDari EverandDistillation Design and Control Using Aspen SimulationPenilaian: 5 dari 5 bintang5/5 (2)
- First U.K. National Conference on Heat Transfer: The Institution of Chemical Engineers Symposium Series, Volume 2.86Dari EverandFirst U.K. National Conference on Heat Transfer: The Institution of Chemical Engineers Symposium Series, Volume 2.86Belum ada peringkat
- Fundamentals of Risk Management for Process Industry EngineersDari EverandFundamentals of Risk Management for Process Industry EngineersBelum ada peringkat
- Fun Facts about Hydrogen : Chemistry for Kids The Element Series | Children's Chemistry BooksDari EverandFun Facts about Hydrogen : Chemistry for Kids The Element Series | Children's Chemistry BooksBelum ada peringkat
- Biotechnology of Metals: Principles, Recovery Methods and Environmental ConcernsDari EverandBiotechnology of Metals: Principles, Recovery Methods and Environmental ConcernsBelum ada peringkat
- Nuclear Energy in the 21st Century: World Nuclear University PressDari EverandNuclear Energy in the 21st Century: World Nuclear University PressPenilaian: 4.5 dari 5 bintang4.5/5 (3)
- The Stress Analysis of Pressure Vessels and Pressure Vessel Components: International Series of Monographs in Mechanical EngineeringDari EverandThe Stress Analysis of Pressure Vessels and Pressure Vessel Components: International Series of Monographs in Mechanical EngineeringS. S. GillPenilaian: 3.5 dari 5 bintang3.5/5 (3)
- Coulson and Richardson’s Chemical Engineering: Volume 2B: Separation ProcessesDari EverandCoulson and Richardson’s Chemical Engineering: Volume 2B: Separation ProcessesAjay Kumar RayBelum ada peringkat