Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Chapter 04 Chemical EquilibriumDokumen150 halamanChapter 04 Chemical Equilibriumnoel100% (6)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Manual Prevention An Control of Lost Cir PDFDokumen222 halamanManual Prevention An Control of Lost Cir PDFAna Maria TovarBelum ada peringkat
- E-Studio 205L, 255, 305, 355, 455 MFP Service HandbookDokumen732 halamanE-Studio 205L, 255, 305, 355, 455 MFP Service HandbookAnonymous gn8qxx66% (35)
- The Mathematical Society of Serbia - 60 YearsDokumen23 halamanThe Mathematical Society of Serbia - 60 YearsBranko Ma Branko TadicBelum ada peringkat
- Flue Gas Analysis in IndustryDokumen150 halamanFlue Gas Analysis in Industryblack_knight728Belum ada peringkat
- Introduction To Chaos: The Damped, Driven, Nonlinear PendulumDokumen14 halamanIntroduction To Chaos: The Damped, Driven, Nonlinear PendulumKikkuBelum ada peringkat
- BMG Idle CatlogueDokumen20 halamanBMG Idle Catloguechintan mistryBelum ada peringkat
- LC08 L1TP 120065 20180318 20180403 01 T1 MTLDokumen4 halamanLC08 L1TP 120065 20180318 20180403 01 T1 MTLrendy aswinBelum ada peringkat
- Energy Audit Report by CPRIDokumen247 halamanEnergy Audit Report by CPRImag_ktps20021520100% (2)
- 7 Market EquilibriumDokumen4 halaman7 Market EquilibriumAdeeba iqbalBelum ada peringkat
- Beration of LightDokumen7 halamanBeration of LightAnonymous i71HvPXBelum ada peringkat
- Battery SubsystemDokumen7 halamanBattery SubsystemahmaborashedBelum ada peringkat
- ReadmeRC8007 PDFDokumen2 halamanReadmeRC8007 PDFمنير أحمدBelum ada peringkat
- Nylon Bag BisDokumen13 halamanNylon Bag Bisbsnl.corp.pbBelum ada peringkat
- HVSI804T WGD 83Dokumen6 halamanHVSI804T WGD 83mnezamiBelum ada peringkat
- La 3391p Rev0.3novo DesbloqueadoDokumen48 halamanLa 3391p Rev0.3novo DesbloqueadoRogeriotabiraBelum ada peringkat
- 13 EGWDC 2012 CompresscoDokumen17 halaman13 EGWDC 2012 CompresscoVeky Pamintu100% (1)
- Section 3 Quiz, Database Design ORACLEDokumen8 halamanSection 3 Quiz, Database Design ORACLEMostragBelum ada peringkat
- Design and Implementation of Audio Transceiver Using Infrared Laser For Audio Signal DetectionDokumen4 halamanDesign and Implementation of Audio Transceiver Using Infrared Laser For Audio Signal DetectionGoitom HaileBelum ada peringkat
- ITTC Surface TreatmentDokumen63 halamanITTC Surface Treatments_brizzolaraBelum ada peringkat
- Physics Investigatory Project On Transformers.Dokumen17 halamanPhysics Investigatory Project On Transformers.sridevikamaraj16Belum ada peringkat
- Infinix NOTE 5 Stylus Quick Guide: Together We Can!Dokumen16 halamanInfinix NOTE 5 Stylus Quick Guide: Together We Can!LescribeurBelum ada peringkat
- Omnibus Risk EstimatorDokumen6 halamanOmnibus Risk EstimatorConta do CerberusBelum ada peringkat
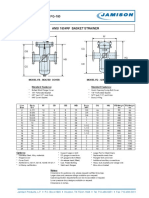
- FB-150 FQ-150 Basket StrainerDokumen1 halamanFB-150 FQ-150 Basket Strainerklich77Belum ada peringkat
- Mac On FigDokumen449 halamanMac On Figvuk_vucko_vukovicBelum ada peringkat
- Pov Nori Apr2007Dokumen31 halamanPov Nori Apr2007DMRBelum ada peringkat
- Coding in Communication System: Channel Coding) Will Be AddressedDokumen5 halamanCoding in Communication System: Channel Coding) Will Be AddressedDuge PlakolliBelum ada peringkat
- 7 - Introduction To Intelligent ControlDokumen21 halaman7 - Introduction To Intelligent ControlIsmael Espinoza100% (1)
- Lec.5 (Prameters of OHTL Pt.2)Dokumen10 halamanLec.5 (Prameters of OHTL Pt.2)AbdullahBelum ada peringkat
- Sensor Gaurd Installation and Maintenance ManualDokumen57 halamanSensor Gaurd Installation and Maintenance ManualCapacitacion TodocatBelum ada peringkat