Anda mungkin juga menyukai
- Masa Simpan TebuDokumen8 halamanMasa Simpan TebuMahesa PriadantaBelum ada peringkat
- RocvaliuDokumen4 halamanRocvaliuFastabiqul KhairatBelum ada peringkat
- Pert 3. Sediaan Radiofarmasi Dan RadiolabelingDokumen19 halamanPert 3. Sediaan Radiofarmasi Dan Radiolabelingwida safitrBelum ada peringkat
- Iohexol USP42NF37Dokumen5 halamanIohexol USP42NF37John Alejandro Restrepo GarciaBelum ada peringkat
- Analisis Deskriptif Efek Samping Penggunaan Obat Anti Tuberculosis Pada Pasien TBC Di Rsud Dr. Pirngadi MedanDokumen7 halamanAnalisis Deskriptif Efek Samping Penggunaan Obat Anti Tuberculosis Pada Pasien TBC Di Rsud Dr. Pirngadi MedanEva MelisaBelum ada peringkat
- Pharmacy Intravena Admixture Services (Pivas) : IV - Admixture Handling CytotoxicDokumen32 halamanPharmacy Intravena Admixture Services (Pivas) : IV - Admixture Handling CytotoxicintanBelum ada peringkat
- Uji Bebas AlkoholDokumen13 halamanUji Bebas AlkoholVieviepunya'esayonggRudii SakmampuseBelum ada peringkat
- Bing DasarDokumen35 halamanBing DasarAfdhal AdolovesoBelum ada peringkat
- Antibiotika RevDokumen55 halamanAntibiotika Revpuspadina ebeBelum ada peringkat
- Coump & Disp (B - Latifah)Dokumen101 halamanCoump & Disp (B - Latifah)Muhammad Nurhadi Bin AbdulghaffarBelum ada peringkat
- Patient Counselling RotahalerDokumen4 halamanPatient Counselling RotahalerJoeann WilsonBelum ada peringkat
- Adverse Drug ReactionDokumen4 halamanAdverse Drug ReactionRahmatulloh Al HusnaBelum ada peringkat
- Kuliah Colon DDS Reguler-Ganjil 2010 INDDokumen125 halamanKuliah Colon DDS Reguler-Ganjil 2010 INDYartiSulistiaNingratBelum ada peringkat
- Usp Bud FactsheetDokumen3 halamanUsp Bud FactsheetdellaBelum ada peringkat
- 2021 Aiphe International Summer School: ChargeDokumen2 halaman2021 Aiphe International Summer School: ChargeAkmalBelum ada peringkat
- 44 85 1 SMDokumen9 halaman44 85 1 SMsilvanaanggraeniBelum ada peringkat
- Dipiro Edisi 9 KolestrolDokumen10 halamanDipiro Edisi 9 KolestrolFriska tampuboLonBelum ada peringkat
- PDF Latihan Soal Ujian Masuk Apoteker Uin Jakarta CompressDokumen20 halamanPDF Latihan Soal Ujian Masuk Apoteker Uin Jakarta CompressTaufiq SibaraniBelum ada peringkat
- Jurnal AlkalinitasDokumen10 halamanJurnal AlkalinitasYunikhe Ana FisyaBelum ada peringkat
- Review Jurnal Sterile CompoundingDokumen6 halamanReview Jurnal Sterile CompoundingAyu BenedictaBelum ada peringkat
- Permasalahan DLM CompoundingDokumen60 halamanPermasalahan DLM CompoundingRusyda Humaira ArumaishaBelum ada peringkat
- Inkompatibilitas 2015Dokumen49 halamanInkompatibilitas 2015Sandy MurtiningtyasBelum ada peringkat
- Modul UKAI 2015 FarmakokimiaDokumen41 halamanModul UKAI 2015 FarmakokimiaBobbyGunarsoBelum ada peringkat
- Daftar Persentase Obat TerdialisisDokumen1 halamanDaftar Persentase Obat Terdialisismazz.rianBelum ada peringkat
- Formularium Apotek TodayDokumen28 halamanFormularium Apotek TodayNora Putri NarindraBelum ada peringkat
- A Review On Film Forming Gel FFGDokumen10 halamanA Review On Film Forming Gel FFGEditor IJTSRDBelum ada peringkat
- Preformulasi AsetosalDokumen2 halamanPreformulasi AsetosalTazyinul Qoriah AlfauziahBelum ada peringkat
- SPO High AlerTDokumen19 halamanSPO High AlerTHendraTriSaputroBelum ada peringkat
- Price List Alkes Pt. Carmella Gustavindo PERIODE JANUARY 2021 (Week 2)Dokumen21 halamanPrice List Alkes Pt. Carmella Gustavindo PERIODE JANUARY 2021 (Week 2)naelarizqiBelum ada peringkat
- Daun LeilemDokumen8 halamanDaun Leilemniken retnoBelum ada peringkat
- Dipiro PneumoniaDokumen8 halamanDipiro Pneumoniameri dayaniBelum ada peringkat
- PERHITUNGAN P2. Studi Absorpsi in Vitro - Usus TerbalikDokumen7 halamanPERHITUNGAN P2. Studi Absorpsi in Vitro - Usus TerbalikDiah AyuBelum ada peringkat
- BISMILLAH LOLOS UKAI 2022 NewDokumen5 halamanBISMILLAH LOLOS UKAI 2022 NewMaya SeptianaBelum ada peringkat
- Transdermal Drug DeliveryDokumen37 halamanTransdermal Drug Deliveryabdullah2020Belum ada peringkat
- 02-Pharmaceutical Care ProcessDokumen42 halaman02-Pharmaceutical Care ProcessBalsam Zahi Al-Hasan100% (1)
- Laporan MonitoringDokumen16 halamanLaporan MonitoringAdi Nak MadiunBelum ada peringkat
- Daftar Harga Buana Saraswati Bulan Agustus PDFDokumen57 halamanDaftar Harga Buana Saraswati Bulan Agustus PDFJasa Sunat JembranaBelum ada peringkat
- DDD Rawat Inap ExcelDokumen10 halamanDDD Rawat Inap ExcelJakobus Benny SalimBelum ada peringkat
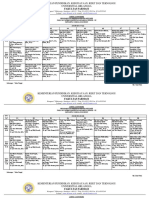
- Jadwal Ujian Sidang Periode 112 TGL 26-27 Juni 2021 (Rev)Dokumen9 halamanJadwal Ujian Sidang Periode 112 TGL 26-27 Juni 2021 (Rev)Yohan Nafisa NetBelum ada peringkat
- Contoh Soal FarmakokinetikDokumen3 halamanContoh Soal FarmakokinetikAina AzkiaBelum ada peringkat
- 1099-1105 Ijpr1301179Dokumen7 halaman1099-1105 Ijpr1301179Indah Indryani UBelum ada peringkat
- Formulasi Dan Evaluasi Sediaan Tablet Asam Mefenamat Menggunakan Eksipien Croscarmellose Sodium Sebagai Disintegran Dengan Metode Granulasi BasahDokumen8 halamanFormulasi Dan Evaluasi Sediaan Tablet Asam Mefenamat Menggunakan Eksipien Croscarmellose Sodium Sebagai Disintegran Dengan Metode Granulasi BasahressyBelum ada peringkat
- TEMPLATE Dan COVERING LETTER JFIKIDokumen8 halamanTEMPLATE Dan COVERING LETTER JFIKItyaBelum ada peringkat
- JurnalDokumen4 halamanJurnallailaBelum ada peringkat
- Prof. Dr. Suharjono, MS., Apt.: STIKES RS Anwar Medika DariDokumen65 halamanProf. Dr. Suharjono, MS., Apt.: STIKES RS Anwar Medika DariYowan SusantiBelum ada peringkat
- Penerapan Farmakoepidemiologi Dalam Praktek KefarmasianDokumen123 halamanPenerapan Farmakoepidemiologi Dalam Praktek KefarmasianRachma DyraBelum ada peringkat
- Idoxuridine 0.5% Ophthalmic OintmentDokumen1 halamanIdoxuridine 0.5% Ophthalmic Ointmentmd_corona62Belum ada peringkat
- Tugas Xii FDokumen9 halamanTugas Xii FNurrochimBelum ada peringkat
- Absolute Bioavailability & Relative Bioavailability PDFDokumen8 halamanAbsolute Bioavailability & Relative Bioavailability PDFNehaBelum ada peringkat
- Soal Apoteker UpertisDokumen27 halamanSoal Apoteker Upertisriri rahmadhani18Belum ada peringkat
- Daftar Obat Aman Dan Berbahaya Untuk Ibu Hamil Dan MenyusuiDokumen28 halamanDaftar Obat Aman Dan Berbahaya Untuk Ibu Hamil Dan MenyusuiDwiPrasetyaningRahmawatiBelum ada peringkat
- MikroenkapsulasiDokumen21 halamanMikroenkapsulasiFadel TrianzahBelum ada peringkat
- Dapus Umum LengkapDokumen6 halamanDapus Umum LengkapDhewiantyBelum ada peringkat
- Dexamethasone Sodium PhosphateDokumen16 halamanDexamethasone Sodium PhosphateMuha Hanafy100% (1)
- Materi 1 Dr. Apt. Diana Laila Ramatillah, M.farmDokumen32 halamanMateri 1 Dr. Apt. Diana Laila Ramatillah, M.farmDimas RfBelum ada peringkat
- Update Stok 04okt2021Dokumen500 halamanUpdate Stok 04okt2021sherly damayantiBelum ada peringkat
- Prof Henny Lucida PHD Apt Calculation of DosespptDokumen27 halamanProf Henny Lucida PHD Apt Calculation of DosespptWella CitraersyaBelum ada peringkat
- AminoglycosidesDokumen55 halamanAminoglycosidesIndira ButkoonBelum ada peringkat
- Calculation of DosesDokumen27 halamanCalculation of DosesAhmad Radhya Dionanda100% (1)
- FAT Soluble VitaminsDokumen53 halamanFAT Soluble VitaminsFaria LatifBelum ada peringkat
- Adult History and Physical Examination Well Patient Encounter (A Checklist For Medical Students)Dokumen13 halamanAdult History and Physical Examination Well Patient Encounter (A Checklist For Medical Students)Michael Harrison Chopade100% (1)
- Burns NeliganDokumen45 halamanBurns NeliganroyvillafrancaBelum ada peringkat
- SEER Lymph Node FieldsDokumen9 halamanSEER Lymph Node FieldsNetradeep Narayansa DagduBelum ada peringkat
- Pixl Knowit!: Gcse BiologyDokumen47 halamanPixl Knowit!: Gcse BiologyLisa MillardBelum ada peringkat
- Stages of LaborDokumen3 halamanStages of Labormiss RN100% (8)
- USNI Medication TestDokumen8 halamanUSNI Medication Testusni100% (31)
- 6 Pap Smear Staining ProeduresDokumen26 halaman6 Pap Smear Staining Proeduresnguyenvu2412100% (2)
- 4th Lecture On Physiology of Eye by Dr. RoomiDokumen36 halaman4th Lecture On Physiology of Eye by Dr. RoomiMudassar RoomiBelum ada peringkat
- AngiogenezaDokumen19 halamanAngiogenezaamaliaanghelBelum ada peringkat
- Partoza, J WS Cel - MolDokumen6 halamanPartoza, J WS Cel - MolJenny PartozaBelum ada peringkat
- Nonnewtonian and Newtonian Blood Flow in Human Aorta A Transient AnalysisDokumen10 halamanNonnewtonian and Newtonian Blood Flow in Human Aorta A Transient AnalysisDivyaVatsBelum ada peringkat
- Photosynthesis Class 10Dokumen14 halamanPhotosynthesis Class 10shreya morajkarBelum ada peringkat
- Rubriblast/ Pronormoblast: Size: Nucleus: Cytoplasm: N:C Ratio: Additional NotesDokumen13 halamanRubriblast/ Pronormoblast: Size: Nucleus: Cytoplasm: N:C Ratio: Additional NotesOsannah Irish InsongBelum ada peringkat
- Full Moon Cockfight - Stevie's Blog Cockfight StoryDokumen4 halamanFull Moon Cockfight - Stevie's Blog Cockfight Storydionne3chan6Belum ada peringkat
- Digestive SystemDokumen30 halamanDigestive SystemImneil Jeanne Melendres-PerezBelum ada peringkat
- Integumentary System - NUR1019 - 20sept2022Dokumen33 halamanIntegumentary System - NUR1019 - 20sept2022琪琪Belum ada peringkat
- DLL - Science 6 - Q2 - W2Dokumen8 halamanDLL - Science 6 - Q2 - W2Shiela RoaBelum ada peringkat
- Ananya Agarwal - BiopsychologyDokumen12 halamanAnanya Agarwal - BiopsychologyANANYA AGARWAL 20224305Belum ada peringkat
- Muscles and Muscle Tissue: Chapter 9 Part ADokumen82 halamanMuscles and Muscle Tissue: Chapter 9 Part ADon KeyBelum ada peringkat
- Nutrition QuizDokumen3 halamanNutrition QuizAnonymous h2EnKyDb100% (1)
- SOP ExerciseTherapy - e - Eng PDFDokumen372 halamanSOP ExerciseTherapy - e - Eng PDFEli WatiBelum ada peringkat
- Acute Phase ProteinsDokumen380 halamanAcute Phase ProteinsRogerio CansiBelum ada peringkat
- Cerebrovascular DiseaseDokumen54 halamanCerebrovascular Diseaselisaagustina100% (1)
- Glossary of Radiology Signs by SystemsDokumen2 halamanGlossary of Radiology Signs by SystemsIssa OliverBelum ada peringkat
- Anat MuscleDokumen164 halamanAnat Musclejohn delaBelum ada peringkat
- IGCSE Answers Chapters 01 05Dokumen7 halamanIGCSE Answers Chapters 01 05María Eugenia MolteniBelum ada peringkat
- Fish Diseases FactsheetDokumen2 halamanFish Diseases FactsheetWayneBelum ada peringkat
- Q. With RationalDokumen102 halamanQ. With RationalDr-Sanjay SinghaniaBelum ada peringkat
- Early Warning ScoresDokumen14 halamanEarly Warning ScoresmuchtarBelum ada peringkat