Anda mungkin juga menyukai
- Sax S Dangerous Properties of Industrial Materials 5 Volume Set PDFDokumen4.795 halamanSax S Dangerous Properties of Industrial Materials 5 Volume Set PDFTom100% (1)
- Pathophysiology of OsteosarcomaDokumen5 halamanPathophysiology of Osteosarcomafanvicfay100% (9)
- Old Photo Respiration Test With Answer KeyDokumen11 halamanOld Photo Respiration Test With Answer KeySamuel SiyumBelum ada peringkat
- Genetics and Epigenetics of Infertility and Treatments On OutcomesDokumen16 halamanGenetics and Epigenetics of Infertility and Treatments On OutcomesCamii Cv100% (1)
- Handbook of Current and Novel Protocols for the Treatment of InfertilityDari EverandHandbook of Current and Novel Protocols for the Treatment of InfertilityMichael H. DahanBelum ada peringkat
- DHEA Final PresentationDokumen140 halamanDHEA Final PresentationSundar Narayanan100% (1)
- Embryology GenitalDokumen53 halamanEmbryology GenitalDhonat Flash100% (1)
- Miscarriages and NutritionDokumen70 halamanMiscarriages and NutritionErwin Ginting100% (2)
- Human Endometrial ReceptivityDokumen39 halamanHuman Endometrial Receptivityrafifah_nadia100% (2)
- PRP Therapy in EndometriumDokumen26 halamanPRP Therapy in Endometriumdrsuryakant9818100% (1)
- Infertility 001Dokumen257 halamanInfertility 001Habtamu Nigussie100% (1)
- Metabolic and Endocrine Pharmacology: Gonadol DrugsDokumen38 halamanMetabolic and Endocrine Pharmacology: Gonadol Drugstheintrov100% (1)
- Fertility NICE GuidelineDokumen51 halamanFertility NICE Guidelineshahryar shaukatBelum ada peringkat
- SBM Reproduction NotesDokumen73 halamanSBM Reproduction NotesAhra100% (2)
- Thin Endometrium: Dr. Astha Gupta Senior Ivf and Infertility Consultant Milann Fertility, DelhiDokumen56 halamanThin Endometrium: Dr. Astha Gupta Senior Ivf and Infertility Consultant Milann Fertility, DelhiDrAstha Gupta100% (1)
- Drugs 2 (Gyneac)Dokumen103 halamanDrugs 2 (Gyneac)Aman Shaikh100% (2)
- The Poor Responder - New Medical TreatmentDokumen35 halamanThe Poor Responder - New Medical TreatmentBrijesh Mishra100% (1)
- Nutrients and Botanicals For Erectile Dysfunction: Examining The EvidenceDokumen13 halamanNutrients and Botanicals For Erectile Dysfunction: Examining The EvidenceChrystian Silva100% (1)
- Presentation 1Dokumen58 halamanPresentation 1Kuch Bhi50% (2)
- Urodynamics For Urogynecologists Vignoli2018Dokumen249 halamanUrodynamics For Urogynecologists Vignoli2018Griselda Pérez Alcántara100% (1)
- Recurrent Implantation Failure-Update Overview OnDokumen19 halamanRecurrent Implantation Failure-Update Overview Onn2763288100% (1)
- Assessment of Fetal WellbeingDokumen177 halamanAssessment of Fetal Wellbeingvrutipatel100% (1)
- Progesterone in PregnancyDokumen59 halamanProgesterone in PregnancyKaruna Indoliya100% (2)
- The Best Foods For Erectile DysfunctionDokumen13 halamanThe Best Foods For Erectile DysfunctionSophia Chloe100% (1)
- First Trimester Screening B Bhagyashree BhijjaragiDokumen27 halamanFirst Trimester Screening B Bhagyashree BhijjaragiSuyajna Joshi100% (1)
- Endometrial Preparation For FET: DR Astha Gupta, Fellow in Reproductive Medicine, IHRDokumen65 halamanEndometrial Preparation For FET: DR Astha Gupta, Fellow in Reproductive Medicine, IHRDrAstha Gupta100% (1)
- Abortus Berulang Trapi Dan PenatalaksanaanDokumen305 halamanAbortus Berulang Trapi Dan PenatalaksanaanMarthinKolelupun100% (2)
- Sry Sex DeterminationDokumen15 halamanSry Sex Determinationapi-528179516100% (1)
- Recommendations For Good Practice in Ultrasound - 062019Dokumen41 halamanRecommendations For Good Practice in Ultrasound - 062019RakhiBelum ada peringkat
- Approaches To Improve Endometrial Receptivity in Case of Repeated Implantation FailuresDokumen17 halamanApproaches To Improve Endometrial Receptivity in Case of Repeated Implantation FailuresAnh Vũ Hồ Ngọc100% (1)
- @ebookmedicin 2019 Epigenetics andDokumen215 halaman@ebookmedicin 2019 Epigenetics andKevin S100% (1)
- Newer Insulin in Diabetic Pregnancy - PPT'Dokumen56 halamanNewer Insulin in Diabetic Pregnancy - PPT'Hemamalini100% (1)
- Menstruation: Learning OutcomesDokumen87 halamanMenstruation: Learning OutcomesKimberly Whitfield (Kim)100% (2)
- Male Repro Problems 2022 With NotesDokumen65 halamanMale Repro Problems 2022 With NotesNikky Silvestre100% (1)
- Acute Fatty Liver Versus HELLPDokumen44 halamanAcute Fatty Liver Versus HELLPrainmaker77771121100% (1)
- The Use of Aromatase Inhibitors in Infertility and GynecologyDokumen9 halamanThe Use of Aromatase Inhibitors in Infertility and Gynecologyalan lowusBelum ada peringkat
- The Endometrial Factor A Reproductive Precision Medicine ApproachDokumen275 halamanThe Endometrial Factor A Reproductive Precision Medicine ApproachErika Rosas100% (1)
- Abdominal Pain in PregnancyDokumen22 halamanAbdominal Pain in Pregnancyapi-3705046Belum ada peringkat
- 1 - ESHRE ET Guideline - Main DocumentDokumen128 halaman1 - ESHRE ET Guideline - Main Documentblack100% (1)
- Tog Journal 2016Dokumen61 halamanTog Journal 2016thevijay007100% (1)
- Step by Step Interventional Ultrasound in Obstetrics and GynaecologyDokumen116 halamanStep by Step Interventional Ultrasound in Obstetrics and GynaecologySahal Beli100% (1)
- Drugs I (Obgy)Dokumen85 halamanDrugs I (Obgy)Aman Shaikh100% (2)
- Contraceptive ImplantsDokumen17 halamanContraceptive ImplantsKingBee1123Belum ada peringkat
- Advanced and Intensive IUI & IVF Training CourseDokumen6 halamanAdvanced and Intensive IUI & IVF Training CourseRadiance hospitalBelum ada peringkat
- Reproductive Endocrinology For Gynaecologist SDokumen356 halamanReproductive Endocrinology For Gynaecologist SFebey Arie Mulya100% (1)
- Fertilisasi Askeb IDokumen19 halamanFertilisasi Askeb IPutry Utami0% (1)
- Pharmacology of Pregnancy - PPT - Dr. Maulana Antian Empitu (Airlangga Medical Faculty)Dokumen51 halamanPharmacology of Pregnancy - PPT - Dr. Maulana Antian Empitu (Airlangga Medical Faculty)rizkyyunitaa15100% (2)
- Induksi Ovulasi RevDokumen38 halamanInduksi Ovulasi RevBambang SulistyoBelum ada peringkat
- 1 Sex DeterminationDokumen30 halaman1 Sex DeterminationNeru Singh100% (1)
- Endometrial Scratch FinalDokumen43 halamanEndometrial Scratch FinalDr. Abha Majumdar100% (2)
- Ovulation DR JRDokumen28 halamanOvulation DR JRtarajanejo100% (1)
- InfertilityDokumen14 halamanInfertilityDrChauhanBelum ada peringkat
- Infertility Lecture FinalDokumen84 halamanInfertility Lecture FinalMohamed Atef Mohamed100% (1)
- Drugs in PregnancyDokumen52 halamanDrugs in Pregnancydarboeb265100% (2)
- Thyroid Disorders in PregnancyDokumen17 halamanThyroid Disorders in PregnancyFemale calmBelum ada peringkat
- Infertility IDokumen36 halamanInfertility Idr_asaleh100% (1)
- Comprehensive Management of PCOS - GPDokumen48 halamanComprehensive Management of PCOS - GPtata maretha100% (1)
- PRP EndometriumDokumen1 halamanPRP Endometriumdrsuryakant9818100% (1)
- Menstrual Disorders and PCOS Webinar EMBRYO FKUI 2022Dokumen49 halamanMenstrual Disorders and PCOS Webinar EMBRYO FKUI 2022angelinputri100% (1)
- Acute Abdomen During Pregnancy BelaynehDokumen47 halamanAcute Abdomen During Pregnancy BelaynehYohannis AsefaBelum ada peringkat
- 2019 Spermatogenesis Biology and Clinical ImplicationsDokumen293 halaman2019 Spermatogenesis Biology and Clinical ImplicationsPricope Elvis100% (1)
- Interpretation of The Semen Analysis and Initial Male Factor ManagementDokumen10 halamanInterpretation of The Semen Analysis and Initial Male Factor ManagementRosangela Mazariegos CastilloBelum ada peringkat
- Lesson 2Dokumen6 halamanLesson 2NguyễnHoàiNamBelum ada peringkat
- Lesson 1Dokumen6 halamanLesson 1NguyễnHoàiNamBelum ada peringkat
- Impacts of Genetically Modified PDFDokumen11 halamanImpacts of Genetically Modified PDFNguyễnHoàiNamBelum ada peringkat
- Gen EngineeringDokumen8 halamanGen Engineeringhasrol_81Belum ada peringkat
- Jistm 2016 01 09 03 PDFDokumen22 halamanJistm 2016 01 09 03 PDFA Shahrizal MuhamadBelum ada peringkat
- 4 - Principles of EcologyDokumen27 halaman4 - Principles of EcologyshanujssBelum ada peringkat
- Biological Clock in Plants PDFDokumen11 halamanBiological Clock in Plants PDFSuresh IndiaBelum ada peringkat
- An Approach To The de Novo Synthesis of LifeDokumen11 halamanAn Approach To The de Novo Synthesis of LifeJohnBelum ada peringkat
- GATE XL 2019 Botany Solved Question PaperDokumen7 halamanGATE XL 2019 Botany Solved Question PaperPranav NathBelum ada peringkat
- General Biology Lab Manual - F2016 PDFDokumen114 halamanGeneral Biology Lab Manual - F2016 PDFDuncan ComptonBelum ada peringkat
- De Barros 2018Dokumen36 halamanDe Barros 2018Eletícia SousaBelum ada peringkat
- Circadian Rhythm NEJMDokumen12 halamanCircadian Rhythm NEJMtjelongBelum ada peringkat
- Electron Transport and Oxidative Phosphorylation: Refer To: Lehninger Principles of Biochemistry (Chapter 19)Dokumen43 halamanElectron Transport and Oxidative Phosphorylation: Refer To: Lehninger Principles of Biochemistry (Chapter 19)Yousef KhallafBelum ada peringkat
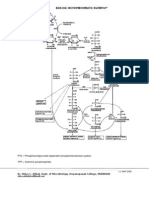
- Hexose Monophosphate Pathway PathwayDokumen3 halamanHexose Monophosphate Pathway PathwayShiva100% (6)
- Yellow Leaf Disease of Sugarcane and Its ManagementDokumen3 halamanYellow Leaf Disease of Sugarcane and Its ManagementNithya KadirvelBelum ada peringkat
- F.Y.B.Sc. Zoology 2019Dokumen12 halamanF.Y.B.Sc. Zoology 2019Sayyad KahekashaBelum ada peringkat
- Virus Vector Relationship & Mites As Vectors of Plant DiseasesDokumen51 halamanVirus Vector Relationship & Mites As Vectors of Plant Diseasesகலியமூர்த்தி செம்மலை80% (5)
- COVID-19 Vaccine Development - Milestones, Lessons and ProspectsDokumen32 halamanCOVID-19 Vaccine Development - Milestones, Lessons and Prospectsnadhia rahdaBelum ada peringkat
- Dna ExtractionDokumen5 halamanDna ExtractionYsabel Francesca AbadBelum ada peringkat
- Paper 1 Midyear Exam Biology Form 4 2010Dokumen18 halamanPaper 1 Midyear Exam Biology Form 4 2010FidaBelum ada peringkat
- THE Cross - Section of A Tree: Prepared By: S. BryanDokumen17 halamanTHE Cross - Section of A Tree: Prepared By: S. BryanBereket BlessingBelum ada peringkat
- FINAL - ALE - An Breeding - GeneticsDokumen71 halamanFINAL - ALE - An Breeding - GeneticsJohana Pinagayao AngkadBelum ada peringkat
- Department of Animal Husbandry and Dairy Science Mahatma Phule Krishi Vidyapeeth Rahuri-413 722, Dist. Ahmednagar (MS)Dokumen20 halamanDepartment of Animal Husbandry and Dairy Science Mahatma Phule Krishi Vidyapeeth Rahuri-413 722, Dist. Ahmednagar (MS)dahiphale1100% (1)
- Programmable Protein Delivery With A Bacterial Contractile Injection System - s41586-023-05870-7Dokumen28 halamanProgrammable Protein Delivery With A Bacterial Contractile Injection System - s41586-023-05870-7vin.vinylBelum ada peringkat
- For Each of The Following Multiple Choice Questions, Select The BEST AnswerDokumen6 halamanFor Each of The Following Multiple Choice Questions, Select The BEST AnswerAbdul Ghaffar AbdullahBelum ada peringkat
- PEE Module 2Dokumen3 halamanPEE Module 2Aki WasakosupBelum ada peringkat
- Mendelian GeneticsDokumen52 halamanMendelian Geneticshengst librandoBelum ada peringkat
- Ethnobotanical Investigation of Three Traditional Leafy Vegetables (Alternanthera Sessilis (L.) DC. Bidens Pilosa L. Launaea Taraxacifolia Willd.) Widely Consumed in Southern and Central BeninDokumen12 halamanEthnobotanical Investigation of Three Traditional Leafy Vegetables (Alternanthera Sessilis (L.) DC. Bidens Pilosa L. Launaea Taraxacifolia Willd.) Widely Consumed in Southern and Central BeninInternational Network For Natural SciencesBelum ada peringkat
- C.V Pinaki BiswasDokumen3 halamanC.V Pinaki BiswasPinaki BiswasBelum ada peringkat
- C 06 From Chromosomes To GenomesDokumen60 halamanC 06 From Chromosomes To GenomesHamadaShehataBelum ada peringkat
- Lesson Preview: Checking For UnderstandingDokumen2 halamanLesson Preview: Checking For UnderstandingKristinelou Marie N. ReynaBelum ada peringkat