Anda mungkin juga menyukai
- Thesis Prop Trial Print BWDokumen18 halamanThesis Prop Trial Print BWOldriana Prawiro HapsariBelum ada peringkat
- Thesis Prop Trial Print BWDokumen18 halamanThesis Prop Trial Print BWOldriana Prawiro HapsariBelum ada peringkat
- Precede/ProceedDokumen10 halamanPrecede/ProceedOldriana Prawiro HapsariBelum ada peringkat
- Precede-Proceed ModelDokumen16 halamanPrecede-Proceed ModelOldriana Prawiro Hapsari100% (1)
- Application of The WHO Keys of Safer Food To Improve Food Handling Practices of Food Vendors in A Poor Resource Community in GhanaDokumen10 halamanApplication of The WHO Keys of Safer Food To Improve Food Handling Practices of Food Vendors in A Poor Resource Community in GhanaOldriana Prawiro HapsariBelum ada peringkat
- Singapore Train System MapDokumen1 halamanSingapore Train System MapOldriana Prawiro HapsariBelum ada peringkat
- RCT of Aprv Vs LPV in Ards PtsDokumen11 halamanRCT of Aprv Vs LPV in Ards PtsOldriana Prawiro HapsariBelum ada peringkat
- Thyroid Disease in PregnancyDokumen12 halamanThyroid Disease in PregnancyOldriana Prawiro HapsariBelum ada peringkat
- Ad and Ar InheritanceDokumen45 halamanAd and Ar InheritanceOldriana Prawiro HapsariBelum ada peringkat
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Brain DeathDokumen1 halamanBrain DeathSeanBelum ada peringkat
- First Aid AssignmentDokumen14 halamanFirst Aid AssignmentJeremy Rei Mendroz100% (1)
- Nasal TraumaDokumen5 halamanNasal TraumaRae Marie AquinoBelum ada peringkat
- Latihan Amali: Wja 102:balutan Ringkas 9 NOVEMBER 2020Dokumen19 halamanLatihan Amali: Wja 102:balutan Ringkas 9 NOVEMBER 2020pei yeu tehBelum ada peringkat
- Feridas Difícil CicatrizaçãoDokumen22 halamanFeridas Difícil CicatrizaçãoBia BerzotiBelum ada peringkat
- Antepartum HaemorrhageDokumen36 halamanAntepartum HaemorrhageAfi RamadaniBelum ada peringkat
- Dahil Sa Tindi NG Kahirapan Sa ProbinsyaDokumen5 halamanDahil Sa Tindi NG Kahirapan Sa ProbinsyaElisha Gine AndalesBelum ada peringkat
- Lunotriquetral CoalitionDokumen3 halamanLunotriquetral Coalitionsuribabu963Belum ada peringkat
- Herniated Nucleus Pulposus (HNP)Dokumen21 halamanHerniated Nucleus Pulposus (HNP)Kaye100% (1)
- The Nameless CityDokumen34 halamanThe Nameless CityThe DoctorBelum ada peringkat
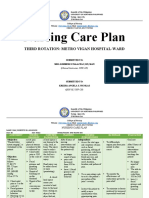
- Nursing Care Plan: Third Rotation: Metro Vigan Hospital-WardDokumen5 halamanNursing Care Plan: Third Rotation: Metro Vigan Hospital-WardKrizha Angela NicolasBelum ada peringkat
- Format Rekapan Elbow Injury 2012-2016Dokumen6 halamanFormat Rekapan Elbow Injury 2012-2016yesaBelum ada peringkat
- Emergency Neurological Life Support - 4th Edition - 1Dokumen33 halamanEmergency Neurological Life Support - 4th Edition - 1Allan HongBelum ada peringkat
- Skeletal System Practice QuizDokumen4 halamanSkeletal System Practice QuizDavid Rosas100% (2)
- 38 MCQs - TORTDokumen7 halaman38 MCQs - TORTmohamed mowafeyBelum ada peringkat
- Carpal Tunnel SyndromeDokumen43 halamanCarpal Tunnel SyndromePra YudhaBelum ada peringkat
- Bone Fracture Detection Through The Two-Stage SystDokumen32 halamanBone Fracture Detection Through The Two-Stage SystSaHiL SiNgHBelum ada peringkat
- Body Empowerment ThoracisExercisesDokumen16 halamanBody Empowerment ThoracisExercisesdracoscribdBelum ada peringkat
- In Service Thoracic OutletDokumen22 halamanIn Service Thoracic Outletapi-549232349Belum ada peringkat
- Paper 8Dokumen40 halamanPaper 8Francisco Javier Luza Ramos100% (1)
- Sciatica and Lumbar Radiculopathy Prolotherapy Treatments PDFDokumen12 halamanSciatica and Lumbar Radiculopathy Prolotherapy Treatments PDFdannisanurmiyaBelum ada peringkat
- OP-10Procedure For Incident Accident Reporting Investigation & AnalysisDokumen9 halamanOP-10Procedure For Incident Accident Reporting Investigation & Analysisfdfddf dfsdfBelum ada peringkat
- Ridgid Model300 Operators ManualDokumen63 halamanRidgid Model300 Operators ManualLuis Manuel Jiménez SalinasBelum ada peringkat
- SEW EX Asynchronous Servo MotersDokumen144 halamanSEW EX Asynchronous Servo Moterswickedness100% (1)
- Samsung GT-E1202 ManualDokumen2 halamanSamsung GT-E1202 ManualjamesBelum ada peringkat
- Anatomy Notes 1:28:2019Dokumen4 halamanAnatomy Notes 1:28:2019Taylor IgnarriBelum ada peringkat
- Navara D40Dokumen352 halamanNavara D40Hard ManBelum ada peringkat
- 9156 Accident Incident Reporting ManualDokumen87 halaman9156 Accident Incident Reporting ManualVitor M R CoelhoBelum ada peringkat
- Musculosceletal Block: Prof - Dr.Dr. Bambang Pardjianto, SPB., Spbp-Re (K)Dokumen32 halamanMusculosceletal Block: Prof - Dr.Dr. Bambang Pardjianto, SPB., Spbp-Re (K)Irsyad Robani WBelum ada peringkat
- Chapter 5Dokumen20 halamanChapter 5Berihu GirmayBelum ada peringkat