Anda mungkin juga menyukai
- Anatomy Exam Review Muscles Innervations VasculatureDokumen27 halamanAnatomy Exam Review Muscles Innervations Vasculaturegdubs215Belum ada peringkat
- Vegetable Freezing ChartDokumen2 halamanVegetable Freezing Chartgdubs215100% (1)
- Renin Angiotensin Aldosterone SystemDokumen1 halamanRenin Angiotensin Aldosterone Systemgdubs215Belum ada peringkat
- Anatomy of AirwaysDokumen6 halamanAnatomy of Airwaysgdubs215Belum ada peringkat
- Important Vertebral Landmarks Level StructureDokumen5 halamanImportant Vertebral Landmarks Level Structuregdubs215Belum ada peringkat
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- AntibioticsDokumen2 halamanAntibioticsSaeed HasanBelum ada peringkat
- Fortified Drops Chart A4 Modified 1pdfpdf 2Dokumen1 halamanFortified Drops Chart A4 Modified 1pdfpdf 2Rubén SepúlvedaBelum ada peringkat
- AntibioticsDokumen2 halamanAntibioticsPGI Custodio, Ed KristianBelum ada peringkat
- 1 Classification of The AntibioticsDokumen5 halaman1 Classification of The AntibioticsRahma WatiBelum ada peringkat
- B Emergence During The COVID 19 Pandemic of I Klebsiella Pneumoniae I ST307 Co Producing KPC 3 and NDM 1 Carbapenemases BDokumen2 halamanB Emergence During The COVID 19 Pandemic of I Klebsiella Pneumoniae I ST307 Co Producing KPC 3 and NDM 1 Carbapenemases BBacteriología AmebpbaBelum ada peringkat
- JKT Surveillance PPRA 2021Dokumen28 halamanJKT Surveillance PPRA 2021priyantoBelum ada peringkat
- Antibiotic GuidelineDokumen11 halamanAntibiotic GuidelineSanjay ShresthaBelum ada peringkat
- Data Pasien TB JuliDokumen42 halamanData Pasien TB JuliTsubbatun NajahBelum ada peringkat
- WHO Antibiotics Not Recommended 2022Dokumen3 halamanWHO Antibiotics Not Recommended 2022mohamad arifBelum ada peringkat
- Principles of Management of MDR-TBDokumen22 halamanPrinciples of Management of MDR-TBGeorge VergheseBelum ada peringkat
- Antibióticos Lecturas PDFDokumen211 halamanAntibióticos Lecturas PDFDiego Francisco Garcia OrtizBelum ada peringkat
- DFSV - (TIN) Antibiotic Detection LimitsDokumen2 halamanDFSV - (TIN) Antibiotic Detection LimitsChevronelleBelum ada peringkat
- Panencefalitis Esclerosante SubagudaDokumen5 halamanPanencefalitis Esclerosante SubagudaVictor Euclides Briones MoralesBelum ada peringkat
- Sejarah Klasifikasi Antibiotik Dewi - 2017Dokumen58 halamanSejarah Klasifikasi Antibiotik Dewi - 2017dr.syafril SpJPBelum ada peringkat
- Leprosy Summary of MedsDokumen1 halamanLeprosy Summary of MedsNikki LegaspiBelum ada peringkat
- 1 s2.0 S0924857922001455 MainDokumen13 halaman1 s2.0 S0924857922001455 MainRobert StryjakBelum ada peringkat
- Antimicrobial Resistance and Clinical Use in Respiratory InfectionsDokumen23 halamanAntimicrobial Resistance and Clinical Use in Respiratory InfectionsWamique IzharBelum ada peringkat
- Anti-Fungal Compound Library (96-Well) : Product DetailsDokumen1 halamanAnti-Fungal Compound Library (96-Well) : Product DetailsSenuke TestBelum ada peringkat
- Kartu StokDokumen120 halamanKartu StokBintangRamadhanBelum ada peringkat
- A Ten Disk Procedure For The Detection of Antibiotic Resistance in EnterobacteriacaeDokumen7 halamanA Ten Disk Procedure For The Detection of Antibiotic Resistance in EnterobacteriacaeNguyen Huu HienBelum ada peringkat
- Mark M Calban MD MPM-HSDDokumen58 halamanMark M Calban MD MPM-HSDZllison Mae Teodoro Mangabat100% (1)
- IECDokumen6 halamanIECThefatRatBelum ada peringkat
- MVG09Dokumen4 halamanMVG09Sondos HarbiehBelum ada peringkat
- Antibiotics and Penicillin Allergy: Contra-Indicated Contra - Indicated Contra - IndicatedDokumen1 halamanAntibiotics and Penicillin Allergy: Contra-Indicated Contra - Indicated Contra - IndicatedJeferson BraxtonBelum ada peringkat
- Chapter 20 Winter 2020Dokumen48 halamanChapter 20 Winter 2020LESLI RODRIGUEZ BENDEZUBelum ada peringkat
- Ppra Ab Terapi PDFDokumen83 halamanPpra Ab Terapi PDFDIONYSIUS BENIBelum ada peringkat
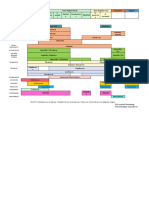
- Ampi+Salbactum Amo+ Clavulanate Piper+Tazobactam: ST ST ND ND ND ND TH ST ND TH TH TH RD RD RD TH THDokumen1 halamanAmpi+Salbactum Amo+ Clavulanate Piper+Tazobactam: ST ST ND ND ND ND TH ST ND TH TH TH RD RD RD TH THAnnieBelum ada peringkat
- Jurnal Pengobatan Empiris Keratitis BakterialDokumen16 halamanJurnal Pengobatan Empiris Keratitis BakterialimuhammadfahmiBelum ada peringkat
- Biology Class Xii Cbse Investigatory Project On AntibioticsDokumen37 halamanBiology Class Xii Cbse Investigatory Project On AntibioticsSaveen Kadian75% (4)