Anda mungkin juga menyukai
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- EC Information Board-FormDokumen1 halamanEC Information Board-FormSARAH MAE MARAVILLABelum ada peringkat
- SRP Batch 1Dokumen32 halamanSRP Batch 1eenahBelum ada peringkat
- Flashcards About Medical DefinitionsDokumen62 halamanFlashcards About Medical DefinitionsSrikanth PagidiBelum ada peringkat
- Assessor Guide EntryLevelSHCODokumen12 halamanAssessor Guide EntryLevelSHCOEka BBelum ada peringkat
- Caroline O'Mahony Caroline's Fit PlanDokumen30 halamanCaroline O'Mahony Caroline's Fit PlanGizem MutluBelum ada peringkat
- Bio MEMSDokumen16 halamanBio MEMStronghuynh12Belum ada peringkat
- Dorothy Johnson PosterDokumen1 halamanDorothy Johnson Posterapi-519455077Belum ada peringkat
- Biological Basis of HomosexulaityDokumen22 halamanBiological Basis of HomosexulaityDhimitri BibolliBelum ada peringkat
- Aira Noreen Leyva - Resume ReviewDokumen2 halamanAira Noreen Leyva - Resume Reviewapi-447475293Belum ada peringkat
- Factors Affecting Demand For Soft DrinksDokumen8 halamanFactors Affecting Demand For Soft Drinksخلود البطاحBelum ada peringkat
- Physical Assessment For Stroke PatientDokumen4 halamanPhysical Assessment For Stroke Patientdana75% (4)
- Big Drugs!!Dokumen2.145 halamanBig Drugs!!Solomon Seth SallforsBelum ada peringkat
- Slu Brochure Ay 2014-2015Dokumen2 halamanSlu Brochure Ay 2014-2015Michael BermudoBelum ada peringkat
- Discrimination in Different FormsDokumen2 halamanDiscrimination in Different FormsPillow ChanBelum ada peringkat
- Edicted PG, StanDokumen69 halamanEdicted PG, StanNwakpa Stanley OgbonnayaBelum ada peringkat
- 478 PeriodizationDokumen13 halaman478 Periodizationomarou1867% (3)
- Req. #1: EMPLOYEES Toyota Workers Say Bosses Have Ignored Safety Concerns For YearsDokumen8 halamanReq. #1: EMPLOYEES Toyota Workers Say Bosses Have Ignored Safety Concerns For YearsbellalitBelum ada peringkat
- Magellan Code ChangesDokumen15 halamanMagellan Code ChangesdaringdreuBelum ada peringkat
- Otto Gross A Case of Exclusion and Oblivion in TheDokumen13 halamanOtto Gross A Case of Exclusion and Oblivion in TheVissente TapiaBelum ada peringkat
- Manual of Homeopathic Practice (1876)Dokumen864 halamanManual of Homeopathic Practice (1876)Dr. JimBelum ada peringkat
- Surgery Alasdair ScottDokumen160 halamanSurgery Alasdair ScottDanny SchBelum ada peringkat
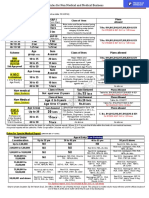
- Rules For Non Medical BusinessDokumen1 halamanRules For Non Medical BusinessAbhijit AminpurBelum ada peringkat
- Boq Lahan Parkir Hotel BogorDokumen2 halamanBoq Lahan Parkir Hotel BogorFariz MemetBelum ada peringkat
- Resolving Therapeutic Alliance Ruptures: Diversity and IntegrationDokumen11 halamanResolving Therapeutic Alliance Ruptures: Diversity and IntegrationPablo GuerraBelum ada peringkat
- Uses of Isotopes in Our Daily LivesDokumen3 halamanUses of Isotopes in Our Daily LivesVibhor Mathur70% (10)
- AP GeographyDokumen95 halamanAP GeographyKhimavathBharathNaik88% (8)
- Delirium Using The 4AT AssessmentDokumen10 halamanDelirium Using The 4AT AssessmentAna KmaidBelum ada peringkat
- Sce550 PresentDokumen57 halamanSce550 Presentapi-289477817Belum ada peringkat
- Risk Assessment: Severity (1, 2 or 3)Dokumen1 halamanRisk Assessment: Severity (1, 2 or 3)Ulviyye ElesgerovaBelum ada peringkat
- Case Study Keme 1Dokumen9 halamanCase Study Keme 1JhovelBelum ada peringkat