Anda mungkin juga menyukai
- Glycogen MetabolismDokumen23 halamanGlycogen Metabolismessa100% (1)
- Pancreatic Islets Hormones Regulate Blood GlucoseDokumen4 halamanPancreatic Islets Hormones Regulate Blood GlucoseSophia OcayBelum ada peringkat
- Glucose Homeostasis and DiabetesDokumen33 halamanGlucose Homeostasis and DiabetesSarahBelum ada peringkat
- Anaerobic Metabolism of Carbohydrates in RBC - Lectue XXIDokumen4 halamanAnaerobic Metabolism of Carbohydrates in RBC - Lectue XXISaulBelum ada peringkat
- Integration of Metabolism: Dr. Farzana Hakim Assistant Professor Biochemistry DepartmentDokumen63 halamanIntegration of Metabolism: Dr. Farzana Hakim Assistant Professor Biochemistry DepartmentGriffinBelum ada peringkat
- Metabolism of Carbohydrate: Department of Biochemistry Faculty of Medicine University of YARSI JakartaDokumen60 halamanMetabolism of Carbohydrate: Department of Biochemistry Faculty of Medicine University of YARSI JakartaAmanda PutriBelum ada peringkat
- 2.2 Carbohydrate Metabolism Part 2Dokumen13 halaman2.2 Carbohydrate Metabolism Part 2John Louis PulidoBelum ada peringkat
- Clinical SignificanceDokumen31 halamanClinical Significancejav israelBelum ada peringkat
- Biochemical Genetics Newborn Screening Population ScreeningDokumen46 halamanBiochemical Genetics Newborn Screening Population ScreeningDrbee10Belum ada peringkat
- Glycogen MetabolismDokumen34 halamanGlycogen MetabolismJomi PorinchuBelum ada peringkat
- Integration of Metabolism PathwaysDokumen68 halamanIntegration of Metabolism PathwaysCahyani Tiara Safitri100% (1)
- Understanding Metabolism of CarbohydratesDokumen48 halamanUnderstanding Metabolism of CarbohydratesAbdullah TheBelum ada peringkat
- Regulation of Growth Hormone SecretionDokumen4 halamanRegulation of Growth Hormone SecretionIbrahim Sugiyono100% (1)
- Uronic Acid PathwayDokumen4 halamanUronic Acid PathwayAlen Arthur100% (2)
- Hormonal Signal TransductionDokumen78 halamanHormonal Signal TransductionNaji Mohamed AlfatihBelum ada peringkat
- GluconeogenesisDokumen48 halamanGluconeogenesisQshyanBelum ada peringkat
- Metabolic Interrelationships Rev 07-11-2014Dokumen82 halamanMetabolic Interrelationships Rev 07-11-2014algutBelum ada peringkat
- Inborn Errors of Metabolism - Basics For Students (Iver Andreas Norbergs Kopi Som Er I Konflikt 2016-01-24)Dokumen4 halamanInborn Errors of Metabolism - Basics For Students (Iver Andreas Norbergs Kopi Som Er I Konflikt 2016-01-24)Wen Jie LauBelum ada peringkat
- Carbohydrate, Lipid, Protein MetabolismDokumen3 halamanCarbohydrate, Lipid, Protein Metabolismtritone.paradoxBelum ada peringkat
- B Y: - Idr. Megha Gaur BDS IDokumen89 halamanB Y: - Idr. Megha Gaur BDS IRishab GaurBelum ada peringkat
- Carbohydrate Storage and Synthesis in Liver and Muscle: GlycogenDokumen40 halamanCarbohydrate Storage and Synthesis in Liver and Muscle: GlycogenJay R PlogioBelum ada peringkat
- PDH Complex and TCA CycleDokumen20 halamanPDH Complex and TCA CycleDarrion LouisBelum ada peringkat
- Endocrine Pancreas & Fuel Homeostasis: Learning ObjectivesDokumen7 halamanEndocrine Pancreas & Fuel Homeostasis: Learning ObjectivesMaggieLockeBelum ada peringkat
- Sella Turcica Releasing Factors Median Eminence Anterior Pituitary Paraventricular Supraoptic NucleiDokumen2 halamanSella Turcica Releasing Factors Median Eminence Anterior Pituitary Paraventricular Supraoptic NucleiDragan Petrovic0% (1)
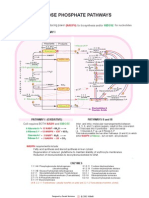
- 21 Pentose Phosphate PathwaysDokumen1 halaman21 Pentose Phosphate Pathwaysİsmail ŞimşekBelum ada peringkat
- Metabolism Lippincott's Q&ADokumen86 halamanMetabolism Lippincott's Q&Alina amjadBelum ada peringkat
- Von Gierke DiseaseDokumen14 halamanVon Gierke Diseaseapi-590506208Belum ada peringkat
- Growth HormonesDokumen42 halamanGrowth Hormonessaputra tri nopianto100% (1)
- Git Biochemistry of GitDokumen9 halamanGit Biochemistry of GitSibatBelum ada peringkat
- CH 19 Integration of MetabolismDokumen63 halamanCH 19 Integration of Metabolismshee140802100% (1)
- Heme Metabolism PDFDokumen19 halamanHeme Metabolism PDFAnonymous jW7BU44ACBelum ada peringkat
- Vitamins ReviewDokumen105 halamanVitamins Reviewjltrek123Belum ada peringkat
- Inborn Errors of MetabolismDokumen4 halamanInborn Errors of Metabolismcurly perkyBelum ada peringkat
- Interconversion of Sugar From Aldose To KetoseDokumen7 halamanInterconversion of Sugar From Aldose To Ketosebeia21Belum ada peringkat
- Chapter 2 P-2 Enzyme-Inhibition 1Dokumen39 halamanChapter 2 P-2 Enzyme-Inhibition 1Raihan I. SakibBelum ada peringkat
- Regulation of Blood Glucose HomeostasisDokumen36 halamanRegulation of Blood Glucose HomeostasiscikcomeBelum ada peringkat
- Biochemistry of Digestive SystemDokumen55 halamanBiochemistry of Digestive SystemSyam UnhasBelum ada peringkat
- Intergration of MetabolismDokumen112 halamanIntergration of MetabolismSantino MajokBelum ada peringkat
- HMPDokumen44 halamanHMPraanja2Belum ada peringkat
- Digestion and Absorption of Carbohydrates: by Arpitha 3 BnysDokumen31 halamanDigestion and Absorption of Carbohydrates: by Arpitha 3 BnysBig ZeroBelum ada peringkat
- 1 Red Blood Cells Anemia and PolycythemiaDokumen43 halaman1 Red Blood Cells Anemia and PolycythemiaGeevee Naganag VentulaBelum ada peringkat
- Glycogen Storage DeseasesDokumen26 halamanGlycogen Storage DeseasesirsaBelum ada peringkat
- Hormonal RegulationDokumen5 halamanHormonal RegulationraizizaBelum ada peringkat
- Citric Acid Cycle Enzyme Pyruvate DehydrogenaseDokumen33 halamanCitric Acid Cycle Enzyme Pyruvate Dehydrogenasesultan khabeeb100% (1)
- Cholesterol and Lipoprotein MetabolismDokumen32 halamanCholesterol and Lipoprotein MetabolismBenjamin PrabhuBelum ada peringkat
- 8 Carbohydrate Metabolism PDFDokumen36 halaman8 Carbohydrate Metabolism PDFDayne Ocampo-SolimanBelum ada peringkat
- Introduction To Endocrinology For Clinical StudentsDokumen28 halamanIntroduction To Endocrinology For Clinical StudentsOhwovoriole ToketemuBelum ada peringkat
- Disorders of Lipid Metabolism LectureDokumen55 halamanDisorders of Lipid Metabolism LectureRichard SiahaanBelum ada peringkat
- SummaryDokumen21 halamanSummarydindaBelum ada peringkat
- Xenobiotic MetabolismDokumen64 halamanXenobiotic MetabolismBelajar dan berdoaBelum ada peringkat
- Biochem Lec Term Paper HypoglycemiaDokumen8 halamanBiochem Lec Term Paper Hypoglycemiaapi-318284296Belum ada peringkat
- Ap Cell Tour 1 ProteinDokumen28 halamanAp Cell Tour 1 Proteinapi-235744933100% (1)
- Fatty Acid Synthesis 11.12.19Dokumen18 halamanFatty Acid Synthesis 11.12.19Sanreet Randhawa100% (1)
- MCQ Carbohydrates Pdffor More JoinDokumen6 halamanMCQ Carbohydrates Pdffor More JoinVikash KushwahaBelum ada peringkat
- Liver Function Test: Prepared By: Siti Norhaiza Binti HadzirDokumen33 halamanLiver Function Test: Prepared By: Siti Norhaiza Binti Hadzirmhafiziab100% (1)
- Porphyrias, Hemoglobinopathies and ThalassemiasDokumen11 halamanPorphyrias, Hemoglobinopathies and ThalassemiasGerald John PazBelum ada peringkat
- Hormon GDSDokumen23 halamanHormon GDSBRI KUBelum ada peringkat
- BiochemIIPart3PPSpring 2011finalDokumen114 halamanBiochemIIPart3PPSpring 2011finalRymma Lukyanenko100% (1)
- AP Position Paper # 1 - Chapter 1Dokumen2 halamanAP Position Paper # 1 - Chapter 1Neel KotrappaBelum ada peringkat
- AP Lang Cause and Effect PaperDokumen3 halamanAP Lang Cause and Effect PaperNeel KotrappaBelum ada peringkat
- Ap Environmental Science - Chapter 5 Crossword PuzzleDokumen2 halamanAp Environmental Science - Chapter 5 Crossword PuzzleNeel KotrappaBelum ada peringkat
- American Dream Essay RoughDokumen2 halamanAmerican Dream Essay RoughNeel Kotrappa100% (1)
- American Dream Essay FinalDokumen4 halamanAmerican Dream Essay FinalNeel Kotrappa100% (1)
- Reparation, Characterization, and Optimization of Microemulsion For Topical Delivery of ItraconazoleDokumen10 halamanReparation, Characterization, and Optimization of Microemulsion For Topical Delivery of ItraconazoleVeni UNBelum ada peringkat
- Trauma Recovery and Empowerment ModelDokumen12 halamanTrauma Recovery and Empowerment Modeljimmiefking_64670597Belum ada peringkat
- Ageing - Physical and Psychological Changes. Pathological Ageing-11!19!2011Dokumen4 halamanAgeing - Physical and Psychological Changes. Pathological Ageing-11!19!2011TaylorBelum ada peringkat
- LPL - Production Test Collection Centre Sector - 18, Block-E Rohini DELHI 110085Dokumen2 halamanLPL - Production Test Collection Centre Sector - 18, Block-E Rohini DELHI 110085Manav ChhabraBelum ada peringkat
- Solution Manual For The Basic Practice of Statistics 8th Edition David S MooreDokumen13 halamanSolution Manual For The Basic Practice of Statistics 8th Edition David S MooreAudreyRayqowjd100% (77)
- Journal of Ethnopharmacology: Shashank Tiwari, Sandeep Kumar Gupta, Anklesh Kumar PathakDokumen8 halamanJournal of Ethnopharmacology: Shashank Tiwari, Sandeep Kumar Gupta, Anklesh Kumar PathakMichael Kohlberger, BSc MScBelum ada peringkat
- Manual of TB and Leprosy in TanzaniaDokumen132 halamanManual of TB and Leprosy in TanzaniaYovanRivanzahBelum ada peringkat
- Hydrochloric Acid MSDSDokumen6 halamanHydrochloric Acid MSDSGia ObligadoBelum ada peringkat
- 2018 VET Product Book PDFDokumen342 halaman2018 VET Product Book PDFToni TodorovBelum ada peringkat
- AUTISM IN CHILDREN: SIGNS, ASSESSMENT AND INTERVENTIONDokumen5 halamanAUTISM IN CHILDREN: SIGNS, ASSESSMENT AND INTERVENTIONvai2Belum ada peringkat
- Caffeine HistoryDokumen9 halamanCaffeine HistoryWynona Genesis G. BasilioBelum ada peringkat
- Coping With Toxic Managers, Subordinates and Other Difficult PeopleDokumen402 halamanCoping With Toxic Managers, Subordinates and Other Difficult Peoplejiggycheng91% (11)
- Sepsis AlgorithmDokumen1 halamanSepsis AlgorithmAshly Nygil100% (1)
- PDFDokumen70 halamanPDFPaul Benjomin AgregadoBelum ada peringkat
- Intro Module1-2a BOSHforSO1 v200806Dokumen57 halamanIntro Module1-2a BOSHforSO1 v200806Elaine GatdulaBelum ada peringkat
- Argumentative EssayDokumen7 halamanArgumentative Essayapi-294732914Belum ada peringkat
- Nutrients: Protein Nutrition and Malnutrition in CKD and ESRDDokumen19 halamanNutrients: Protein Nutrition and Malnutrition in CKD and ESRDrandy_27995Belum ada peringkat
- Rabipur - (EMC) Print FriendlyDokumen8 halamanRabipur - (EMC) Print Friendlyshreyas_chandor3802Belum ada peringkat
- COVID-19 Vaccination Certificate from India's Ministry of HealthDokumen1 halamanCOVID-19 Vaccination Certificate from India's Ministry of Healthbliss bBelum ada peringkat
- 2 02-Electrocardiography PDFDokumen17 halaman2 02-Electrocardiography PDFMiguel DomingoBelum ada peringkat
- 17-Ebcpg Thyroid2013Dokumen20 halaman17-Ebcpg Thyroid2013Mi MingkaiBelum ada peringkat
- A Global Resource For Genomic Predictions of Antimicrobial Resistance and Surveillance of Salmonella Typhi at PathogenwatchDokumen12 halamanA Global Resource For Genomic Predictions of Antimicrobial Resistance and Surveillance of Salmonella Typhi at PathogenwatchOkeke UcheeBelum ada peringkat
- CL142 Environmental Science: Unit: 8 Water PollutionDokumen32 halamanCL142 Environmental Science: Unit: 8 Water PollutionGaurav KapseBelum ada peringkat
- Certificate of Accreditation: Swift Silliker (Pty) LTDDokumen10 halamanCertificate of Accreditation: Swift Silliker (Pty) LTDpham xuan tinh tinhBelum ada peringkat
- Ave Lox TabsDokumen5 halamanAve Lox Tabslrdn_ghrcBelum ada peringkat
- AOAC Rapid Method ValidationDokumen60 halamanAOAC Rapid Method ValidationPiruzi MaghlakelidzeBelum ada peringkat
- Parameters of Mechanics of BreathingDokumen16 halamanParameters of Mechanics of BreathingKaioBelum ada peringkat
- Prak Ospe PK FMS 3 2021Dokumen7 halamanPrak Ospe PK FMS 3 2021Angelique NatalieBelum ada peringkat
- Klenner Protocol For 2013Dokumen10 halamanKlenner Protocol For 2013jcoppala4476Belum ada peringkat
- Universal Credit Work Capability QuestionnaireDokumen24 halamanUniversal Credit Work Capability QuestionnaireSteven Preece100% (2)