Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Robbie Hemingway - Text God VIP EbookDokumen56 halamanRobbie Hemingway - Text God VIP EbookKylee0% (1)
- FMO ESG Toolkit (AutoRecovered)Dokumen149 halamanFMO ESG Toolkit (AutoRecovered)me.abhishekpBelum ada peringkat
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Computer in Community Pharmacy by Adnan Sarwar ChaudharyDokumen10 halamanComputer in Community Pharmacy by Adnan Sarwar ChaudharyDr-Adnan Sarwar Chaudhary100% (1)
- Best of The Photo DetectiveDokumen55 halamanBest of The Photo DetectiveSazeed Hossain100% (3)
- Huruf InjeksiDokumen1 halamanHuruf InjeksiNovella MannuelaBelum ada peringkat
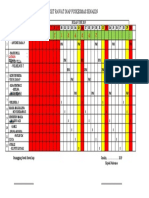
- Jadwal Piket Rawat Inap Puskesmas Senakin: I S T I R A H A TDokumen1 halamanJadwal Piket Rawat Inap Puskesmas Senakin: I S T I R A H A TNovella MannuelaBelum ada peringkat
- Jadwal JuniDokumen1 halamanJadwal JuniNovella MannuelaBelum ada peringkat
- Jadwal JuniDokumen1 halamanJadwal JuniNovella MannuelaBelum ada peringkat
- LidocaineDokumen3 halamanLidocaineNovella MannuelaBelum ada peringkat
- Apoteker Di PuskesmasDokumen10 halamanApoteker Di Puskesmasdeny_flavonoidBelum ada peringkat
- 04 P070 23867Dokumen11 halaman04 P070 23867Novella MannuelaBelum ada peringkat
- Development and Enhancement of Entrapment Efficiency of Isoniazid Loaded Poly - Caprolactone NanoparticleDokumen8 halamanDevelopment and Enhancement of Entrapment Efficiency of Isoniazid Loaded Poly - Caprolactone NanoparticleNovella MannuelaBelum ada peringkat
- Muhammad Gunawan: Penggunaan Gel Kitosan Secara Topikal Efek Penyembuhan..., 2005. USU E-Repository © 2008Dokumen181 halamanMuhammad Gunawan: Penggunaan Gel Kitosan Secara Topikal Efek Penyembuhan..., 2005. USU E-Repository © 2008Novella MannuelaBelum ada peringkat
- Muhammad Gunawan: Penggunaan Gel Kitosan Secara Topikal Efek Penyembuhan..., 2005. USU E-Repository © 2008Dokumen181 halamanMuhammad Gunawan: Penggunaan Gel Kitosan Secara Topikal Efek Penyembuhan..., 2005. USU E-Repository © 2008Novella MannuelaBelum ada peringkat
- Original Article Acne Bangladesh FinalDokumen5 halamanOriginal Article Acne Bangladesh FinalNovella MannuelaBelum ada peringkat
- Chitosan Mediated Targeted Drug DeliveryDokumen22 halamanChitosan Mediated Targeted Drug DeliveryNovella MannuelaBelum ada peringkat
- 139 145 1 PBDokumen10 halaman139 145 1 PBTriansyah PuteraBelum ada peringkat
- Uji DPPHDokumen11 halamanUji DPPHAldila Ratna OvrisadinitaBelum ada peringkat
- Jurnal 2 PDFDokumen17 halamanJurnal 2 PDFNovella MannuelaBelum ada peringkat
- Chemical Classification of HormonesDokumen65 halamanChemical Classification of HormonesetBelum ada peringkat
- Straw Bale ConstructionDokumen37 halamanStraw Bale ConstructionelissiumBelum ada peringkat
- PDFDokumen3 halamanPDFvaliBelum ada peringkat
- Template Remarks For IIDokumen18 halamanTemplate Remarks For IIjasleeneceBelum ada peringkat
- Korea Times - Korean-EnglishDokumen313 halamanKorea Times - Korean-EnglishgyeryongBelum ada peringkat
- Singer 900 Series Service ManualDokumen188 halamanSinger 900 Series Service ManualGinny RossBelum ada peringkat
- Engineering Mathematics John BirdDokumen89 halamanEngineering Mathematics John BirdcoutnawBelum ada peringkat
- E9 Đề khảo sát Trưng Vương 2022 ex No 1Dokumen4 halamanE9 Đề khảo sát Trưng Vương 2022 ex No 1Minh TiếnBelum ada peringkat
- Gothic ArchitectureDokumen6 halamanGothic ArchitectureleeBelum ada peringkat
- The Fluency Course Teacher Instructions PDFDokumen9 halamanThe Fluency Course Teacher Instructions PDFGabriel da RochaBelum ada peringkat
- Facultybooklet2011-2012final - 006 (Unlocked by WWW - Freemypdf.com)Dokumen199 halamanFacultybooklet2011-2012final - 006 (Unlocked by WWW - Freemypdf.com)kalam19892209Belum ada peringkat
- HUAWEI PowerCube 500Dokumen41 halamanHUAWEI PowerCube 500soumen95Belum ada peringkat
- A Summer Training ReportDokumen39 halamanA Summer Training ReportShubham SainyBelum ada peringkat
- Vignyapan 18-04-2024Dokumen16 halamanVignyapan 18-04-2024adil1787Belum ada peringkat
- Fike ECARO-25 Frequently Asked Questions (FAQ)Dokumen8 halamanFike ECARO-25 Frequently Asked Questions (FAQ)Jubert RaymundoBelum ada peringkat
- Bakteri Anaerob: Morfologi, Fisiologi, Epidemiologi, Diagnosis, Pemeriksaan Sy. Miftahul El J.TDokumen46 halamanBakteri Anaerob: Morfologi, Fisiologi, Epidemiologi, Diagnosis, Pemeriksaan Sy. Miftahul El J.TAlif NakyukoBelum ada peringkat
- Material Safety Data Sheet: - AdsealDokumen12 halamanMaterial Safety Data Sheet: - Adsealwuhan lalalaBelum ada peringkat
- Activity Sheet Housekeeping Week - 8 - Grades 9-10Dokumen5 halamanActivity Sheet Housekeeping Week - 8 - Grades 9-10Anne AlejandrinoBelum ada peringkat
- 1000 KilosDokumen20 halaman1000 KilosAbdullah hayreddinBelum ada peringkat
- CAMEL Model With Detailed Explanations and Proper FormulasDokumen4 halamanCAMEL Model With Detailed Explanations and Proper FormulasHarsh AgarwalBelum ada peringkat
- Harley Davidson U S Reportedly Uses Risk Sharing Agreements With Its Foreign SubsidiariesDokumen1 halamanHarley Davidson U S Reportedly Uses Risk Sharing Agreements With Its Foreign Subsidiariestrilocksp SinghBelum ada peringkat
- Business Plan - A TeahouseDokumen6 halamanBusiness Plan - A TeahouseJoe DBelum ada peringkat
- Advanced Statistical Approaches To Quality: INSE 6220 - Week 4Dokumen44 halamanAdvanced Statistical Approaches To Quality: INSE 6220 - Week 4picalaBelum ada peringkat
- Bloomsbury Fashion Central - Designing Children's WearDokumen16 halamanBloomsbury Fashion Central - Designing Children's WearANURAG JOSEPHBelum ada peringkat
- D15 Hybrid P1 QPDokumen6 halamanD15 Hybrid P1 QPShaameswary AnnadoraiBelum ada peringkat
- Amine Processing Unit DEADokumen9 halamanAmine Processing Unit DEAFlorin Daniel AnghelBelum ada peringkat