Anda mungkin juga menyukai
- CAPE Unit 2 Pure Maths NotesDokumen103 halamanCAPE Unit 2 Pure Maths NotesAltrupassionate girlBelum ada peringkat
- Combinatorics 2 Solutions UHSMCDokumen5 halamanCombinatorics 2 Solutions UHSMCWalker KroubalkianBelum ada peringkat
- Unit IV. Solid Modified Release Dosage FormsDokumen24 halamanUnit IV. Solid Modified Release Dosage FormsMary-Ann Valencia SapnuBelum ada peringkat
- Pharmaceutical Dosage Forms Disperse Systems Volume 2Dokumen489 halamanPharmaceutical Dosage Forms Disperse Systems Volume 2Mariana RibeiroBelum ada peringkat
- CulvertsDokumen14 halamanCulvertsMatsobane LekalaksBelum ada peringkat
- Formulation and Evaluation of Effervescent TabletsDokumen8 halamanFormulation and Evaluation of Effervescent TabletsKharisah AfifahBelum ada peringkat
- Extended Release Formulation: Available Online ThroughDokumen60 halamanExtended Release Formulation: Available Online ThroughSomasundaram JeevanandhamBelum ada peringkat
- NDX DolsonDokumen67 halamanNDX DolsonMahanta BorahBelum ada peringkat
- Anti-Aging Therapeutics Volume XIVDari EverandAnti-Aging Therapeutics Volume XIVPenilaian: 3 dari 5 bintang3/5 (1)
- Sustained Controlled ReleaseDokumen43 halamanSustained Controlled Releasesukanya100% (1)
- Tablet: Types of TabletsDokumen82 halamanTablet: Types of TabletsKema Akma100% (1)
- Sustained Release Drug Delivery System - A ReviewDokumen14 halamanSustained Release Drug Delivery System - A ReviewPranav PatelBelum ada peringkat
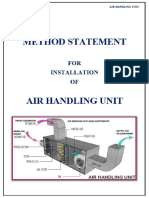
- Method Statement Installation of Air Handling UntDokumen6 halamanMethod Statement Installation of Air Handling UntkouarBelum ada peringkat
- Chapter 9Dokumen66 halamanChapter 9Geline Anne BenozaBelum ada peringkat
- Pharmaceutical Dosage Forms: Disperse Systems, Volume 2Dokumen489 halamanPharmaceutical Dosage Forms: Disperse Systems, Volume 2Sujeevan Kumar Peru77% (22)
- Sustained-Controlled Release DDSDokumen52 halamanSustained-Controlled Release DDSUsama NaushahiBelum ada peringkat
- SUPACDokumen33 halamanSUPACroh12100% (4)
- Handbook of Drug Interaction and the Mechanism of InteractionDari EverandHandbook of Drug Interaction and the Mechanism of InteractionPenilaian: 1 dari 5 bintang1/5 (1)
- Mathematics 9 DLPDokumen10 halamanMathematics 9 DLPAljohaila GulamBelum ada peringkat
- Rectal SuppositoriesDokumen6 halamanRectal SuppositoriesLinh PhamBelum ada peringkat
- Illness Narratives - Positioned IdentitiesDokumen35 halamanIllness Narratives - Positioned IdentitiesAnaBelum ada peringkat
- ParenteralDokumen10 halamanParenteralAbigail Mayled LausBelum ada peringkat
- Tablet KompresiDokumen9 halamanTablet KompresiRatuBelum ada peringkat
- A Prolonged Release Parenteral Drug Delivery SystemDokumen11 halamanA Prolonged Release Parenteral Drug Delivery SystemronnymcmBelum ada peringkat
- Different Aspects of Pellets Formulation and Their Evaluation PDFDokumen6 halamanDifferent Aspects of Pellets Formulation and Their Evaluation PDFHely PatelBelum ada peringkat
- IJCRT23A5406Dokumen19 halamanIJCRT23A5406Agnes Dwi AgithaBelum ada peringkat
- Parenteral Suspension An OverviewDokumen10 halamanParenteral Suspension An OverviewIrma LaumbuBelum ada peringkat
- Formulation and Evaluation of Sustained Release Tablet of Aceclofenac by Film CoatingDokumen9 halamanFormulation and Evaluation of Sustained Release Tablet of Aceclofenac by Film CoatingQoriBelum ada peringkat
- Inlay Tablets A Novel Approach PDFDokumen10 halamanInlay Tablets A Novel Approach PDFTakeshi MondaBelum ada peringkat
- Formulation and Evaluation of Multiunit Pellet System of Venlafaxine HydrochlorideDokumen12 halamanFormulation and Evaluation of Multiunit Pellet System of Venlafaxine HydrochloridevbadsBelum ada peringkat
- DDR SDRAM Controller IP Designed For ReuseDokumen50 halamanDDR SDRAM Controller IP Designed For ReusejagruthimsBelum ada peringkat
- Controlled Drug DeliveryDokumen23 halamanControlled Drug DeliveryAnburaj JamesBelum ada peringkat
- Pharmaceutical Suspensions - PDFDokumen59 halamanPharmaceutical Suspensions - PDFGopalaKrishnan Sivaraman100% (2)
- Pharmaceutical Issues When Crushing, Opening or Splitting Oral Dosage FormsDokumen7 halamanPharmaceutical Issues When Crushing, Opening or Splitting Oral Dosage FormsMohamed OmerBelum ada peringkat
- A Prolonged Release Parenteral Drug Delivery System - An OverviewDokumen11 halamanA Prolonged Release Parenteral Drug Delivery System - An Overviewcristian135Belum ada peringkat
- Abstract:: Extended Release Tablet With Active CoatingDokumen10 halamanAbstract:: Extended Release Tablet With Active Coatingiloveit52252Belum ada peringkat
- Sublingual Drug Delivery SystemDokumen6 halamanSublingual Drug Delivery SystemHely PatelBelum ada peringkat
- Review ArticleDokumen9 halamanReview ArticlemickydivyaBelum ada peringkat
- 12 Chapter 1Dokumen67 halaman12 Chapter 1Michael Ballacky100% (1)
- Makalah Farmasetika Dasar MDRDokumen10 halamanMakalah Farmasetika Dasar MDRWinda WindaBelum ada peringkat
- A Review On Extended Release Drug Delivery SystemDokumen9 halamanA Review On Extended Release Drug Delivery SystemTuyến Đặng ThịBelum ada peringkat
- PhytosomesDokumen25 halamanPhytosomeskondamuri pushpalathaBelum ada peringkat
- Inlay Tablet: A Novel Approach in Oral Drug DeliveryDokumen12 halamanInlay Tablet: A Novel Approach in Oral Drug DeliveryIJAR JOURNALBelum ada peringkat
- Tablets by Yousif Kamal Alternate Edition-2 PDFDokumen14 halamanTablets by Yousif Kamal Alternate Edition-2 PDFSuraj PatelBelum ada peringkat
- Manufacturing: Capsule, A Form of Dosage Form in Medication, Are Common in Our Day-To-Day HealthDokumen3 halamanManufacturing: Capsule, A Form of Dosage Form in Medication, Are Common in Our Day-To-Day HealthZubair Bashir KhanBelum ada peringkat
- Parenteral Suspension: An Overview: International Journal of Current Pharmaceutical ResearchDokumen10 halamanParenteral Suspension: An Overview: International Journal of Current Pharmaceutical ResearchAnonymous 7r2h3YViBelum ada peringkat
- Drug Delivery SystemDokumen15 halamanDrug Delivery SystemC-Net WorksBelum ada peringkat
- 698 PDF PDFDokumen8 halaman698 PDF PDFMuh Indra SudirjaBelum ada peringkat
- MucoadhesifDokumen26 halamanMucoadhesifFeny RafnasariBelum ada peringkat
- Topical and Transdermal Drug Products-Product Quality Tests 3 Drug Release 724Dokumen14 halamanTopical and Transdermal Drug Products-Product Quality Tests 3 Drug Release 724Rara WulansariBelum ada peringkat
- AssignmentDokumen9 halamanAssignmentAbdulbaqi Al AliBelum ada peringkat
- Desired Characteristics and Applications of SuspensionsDokumen8 halamanDesired Characteristics and Applications of Suspensionsasad bashirBelum ada peringkat
- SRDDS Matrix TabletDokumen17 halamanSRDDS Matrix TabletMISBAH KAUSARBelum ada peringkat
- Jurnal TabletDokumen7 halamanJurnal TabletVionaBelum ada peringkat
- Modified-Release Dosage Forms and Drug Delevery SystemsDokumen52 halamanModified-Release Dosage Forms and Drug Delevery SystemsFria Mariz SuperalesBelum ada peringkat
- Buccal Films ThesisDokumen8 halamanBuccal Films Thesistsfublhld100% (2)
- Article WJPR 1467266667Dokumen10 halamanArticle WJPR 1467266667Atthapu ThirupathaiahBelum ada peringkat
- Final Synopsis PHDDokumen13 halamanFinal Synopsis PHDKishor KanaseBelum ada peringkat
- A Short Review On "A Novel Approach in Oral Fast Dissolving Drug Delivery System and Their Patents"Dokumen13 halamanA Short Review On "A Novel Approach in Oral Fast Dissolving Drug Delivery System and Their Patents"Arman DalalBelum ada peringkat
- Ijps258 269Dokumen12 halamanIjps258 269Kristine Dwi PuspitasariBelum ada peringkat
- Dissolution AppartusDokumen11 halamanDissolution AppartusAbdu K. ÊlmankoryBelum ada peringkat
- Hand Out To Students Suspension1Dokumen18 halamanHand Out To Students Suspension1umarBelum ada peringkat
- Immediate Drug Release Dosage Form: A Review: KeywordsDokumen13 halamanImmediate Drug Release Dosage Form: A Review: KeywordsvishalBelum ada peringkat
- Implantable Therapeutic Systems: Introduction of ImplantDokumen16 halamanImplantable Therapeutic Systems: Introduction of ImplantUma MaheswararaoBelum ada peringkat
- Article Wjpps 1408969434Dokumen20 halamanArticle Wjpps 1408969434guptaranjeet40Belum ada peringkat
- Bio AvailabilityDokumen12 halamanBio AvailabilityGnan ChanduBelum ada peringkat
- DOCUMENTA INDICA III - 1553 TO 1557 - mdp-39015019106668-1676484756Dokumen967 halamanDOCUMENTA INDICA III - 1553 TO 1557 - mdp-39015019106668-1676484756roh12Belum ada peringkat
- DOCUMENTA INDICA VI - 1563 TO 1566 - mdp-39015078389015-1676459602Dokumen941 halamanDOCUMENTA INDICA VI - 1563 TO 1566 - mdp-39015078389015-1676459602roh12Belum ada peringkat
- DOCUMENTA INDICA V - 1561 TO 1563 - mdp-39015040793971-1676522485Dokumen921 halamanDOCUMENTA INDICA V - 1561 TO 1563 - mdp-39015040793971-1676522485roh12Belum ada peringkat
- DOCUMENTA INDICA IX - 1573 To 1575 - mdp-39015014313038-1676630388Dokumen861 halamanDOCUMENTA INDICA IX - 1573 To 1575 - mdp-39015014313038-1676630388roh12Belum ada peringkat
- Coatings For ParenteralDokumen7 halamanCoatings For Parenteralroh12Belum ada peringkat
- DOCUMENTA INDICA II - 1550 TO 1553 - mdp-39015014313061-1676484169Dokumen733 halamanDOCUMENTA INDICA II - 1550 TO 1553 - mdp-39015014313061-1676484169roh12Belum ada peringkat
- Technologies - Supplies & Services For The Oncology Market From EvonikDokumen1 halamanTechnologies - Supplies & Services For The Oncology Market From Evonikroh12Belum ada peringkat
- Cryogenics Opps Conference 12-11-14 Rob DoneDokumen42 halamanCryogenics Opps Conference 12-11-14 Rob Doneroh12Belum ada peringkat
- Ophthalmic Products PresentationDokumen19 halamanOphthalmic Products Presentationroh12Belum ada peringkat
- Nda and AndaDokumen21 halamanNda and AndaPavan KumarBelum ada peringkat
- Limited Competitive Examination For IPS, 2012Dokumen5 halamanLimited Competitive Examination For IPS, 2012Voice NgoBelum ada peringkat
- Nda and AndaDokumen21 halamanNda and AndaPavan KumarBelum ada peringkat
- Nda and AndaDokumen21 halamanNda and AndaPavan KumarBelum ada peringkat
- Limited Competitive Examination For IPS, 2012Dokumen5 halamanLimited Competitive Examination For IPS, 2012Voice NgoBelum ada peringkat
- MAS2014Dokumen257 halamanMAS2014Nathaly Rojas GonzálezBelum ada peringkat
- Scaffold 2Dokumen3 halamanScaffold 2Mahmoud Elsayed MohamedBelum ada peringkat
- Humanistic TheoryDokumen28 halamanHumanistic TheoryNano KaBelum ada peringkat
- Foundations For Low Loss GRIN Fiber CouplingDokumen16 halamanFoundations For Low Loss GRIN Fiber CouplingpsylabsBelum ada peringkat
- Akshay Urja Full PDFDokumen56 halamanAkshay Urja Full PDFNeelam Shrivastava100% (2)
- An Exploration of The Concept of Identity Crisis in Salman Rushdie's GrimusDokumen3 halamanAn Exploration of The Concept of Identity Crisis in Salman Rushdie's GrimusIJELS Research JournalBelum ada peringkat
- English Solved SP3Dokumen6 halamanEnglish Solved SP3Prem PatelBelum ada peringkat
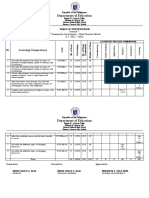
- Department of Education: Learning CompetencyDokumen2 halamanDepartment of Education: Learning CompetencyShaira May Tangonan CaragBelum ada peringkat
- Cars MasonryDokumen1 halamanCars MasonryAbdullah MundasBelum ada peringkat
- Solar Ifc ReportDokumen40 halamanSolar Ifc ReportSIVA NAGA SUDHEER SIDDANIBelum ada peringkat
- Reducing Streetism: A Neglected Cause of Social Anxiety and Delinquency in Adama CityDokumen25 halamanReducing Streetism: A Neglected Cause of Social Anxiety and Delinquency in Adama CityKorie ArsieBelum ada peringkat
- Edit Resume - My Perfect Resume 1Dokumen1 halamanEdit Resume - My Perfect Resume 1Ferid MemmedzadeBelum ada peringkat
- FS 2 - Learning Episode 4-7Dokumen3 halamanFS 2 - Learning Episode 4-7dave puertollanoBelum ada peringkat
- Topic 2.9 WorksheetDokumen3 halamanTopic 2.9 WorksheethaniaBelum ada peringkat
- Ficha Tecnica: KN 95 (Non - Medical)Dokumen13 halamanFicha Tecnica: KN 95 (Non - Medical)Luis Buitrón RamírezBelum ada peringkat
- 5 Đề Thi Giữa Học Kì 2 Môn Tiếng Anh 10 Ilearn Smart World Năm Học 2022-2023 (Có File Nghe)Dokumen48 halaman5 Đề Thi Giữa Học Kì 2 Môn Tiếng Anh 10 Ilearn Smart World Năm Học 2022-2023 (Có File Nghe)Dạy Kèm Quy Nhơn OfficialBelum ada peringkat
- 2347-Article Text-7179-1-10-20220922Dokumen12 halaman2347-Article Text-7179-1-10-20220922george weafriBelum ada peringkat
- Prac Res Q2 Module 8Dokumen12 halamanPrac Res Q2 Module 8Benicel Lane De VeraBelum ada peringkat
- Answers 2Dokumen4 halamanAnswers 2Vika BodokiaBelum ada peringkat
- Genomic and CDNA LibrariesDokumen15 halamanGenomic and CDNA LibrariesPrabhleen KaurBelum ada peringkat
- MRR1Dokumen3 halamanMRR1Shaena LarezaBelum ada peringkat
- VedicReport7 25 20213 48 52PMDokumen55 halamanVedicReport7 25 20213 48 52PMAbhishek BiswalBelum ada peringkat
- Thermodynamics JAM 2021 1Dokumen42 halamanThermodynamics JAM 2021 1krishna prasad ghanta100% (2)