Anda mungkin juga menyukai
- Methods of Western State Secret Services in 1998-2008: Use of Stooges (Patsies), Stalking with Cars, Sleep Deprivation, Toxins, and PainDari EverandMethods of Western State Secret Services in 1998-2008: Use of Stooges (Patsies), Stalking with Cars, Sleep Deprivation, Toxins, and PainBelum ada peringkat
- ELECTROMAGNETIC FIELDS: Exposure is not optional, no one can avoid itDari EverandELECTROMAGNETIC FIELDS: Exposure is not optional, no one can avoid itBelum ada peringkat
- Silent Guardian™ Protection SystemDokumen2 halamanSilent Guardian™ Protection SystemEn MahaksapatalikaBelum ada peringkat
- Stun GunsDokumen6 halamanStun Gunsdefensetechs100% (1)
- Strahlenfolter - Targeted Individual - Viva La Harry - V2K - Gang Stalking - YoutubeDokumen5 halamanStrahlenfolter - Targeted Individual - Viva La Harry - V2K - Gang Stalking - YoutubeGustav-SchneeclausBelum ada peringkat
- Strahlenfolter Stalking - TI - V2K - RNM Remote Neural Monitoring Satellite Terrorism - October 2010 - Satelliteterrorism3.Blogspot - deDokumen5 halamanStrahlenfolter Stalking - TI - V2K - RNM Remote Neural Monitoring Satellite Terrorism - October 2010 - Satelliteterrorism3.Blogspot - deKurt-Schneider100% (1)
- The Structure & Functioning of The Nervous SystemDokumen177 halamanThe Structure & Functioning of The Nervous SystemISHITA GOEL 19224115Belum ada peringkat
- BBC How Long Will Life LastDokumen21 halamanBBC How Long Will Life LastLamantT100% (1)
- Strahlenfolter Stalking - TI - V2K - Can A Satellite Read Your Thoughts - Physics RevealedDokumen6 halamanStrahlenfolter Stalking - TI - V2K - Can A Satellite Read Your Thoughts - Physics RevealedKurt-SchneiderBelum ada peringkat
- Strahlenfolter - Mind Control - Electronic Harassment - WWW - Us-Government-TortureDokumen16 halamanStrahlenfolter - Mind Control - Electronic Harassment - WWW - Us-Government-Torturenwo-mengele-doctorsBelum ada peringkat
- Short Detail of RNM UserDokumen2 halamanShort Detail of RNM UserKunalBelum ada peringkat
- 20210101-PRESS RELEASE MR G. H. Schorel-Hlavka O.W.B. ISSUE - The World Wide 'White' Colour Revolution We Have To Have-Suppl 2Dokumen10 halaman20210101-PRESS RELEASE MR G. H. Schorel-Hlavka O.W.B. ISSUE - The World Wide 'White' Colour Revolution We Have To Have-Suppl 2Gerrit Hendrik Schorel-HlavkaBelum ada peringkat
- GBPPR 'Zine - Issue #62Dokumen76 halamanGBPPR 'Zine - Issue #62GBPPRBelum ada peringkat
- 20210826-Mr G. H. Schorel-Hlavka O.W.B. To Stephanie Brenker BarristerDokumen16 halaman20210826-Mr G. H. Schorel-Hlavka O.W.B. To Stephanie Brenker BarristerGerrit Hendrik Schorel-HlavkaBelum ada peringkat
- WWW Citizensaht Org Implant TechDokumen30 halamanWWW Citizensaht Org Implant TechLazlo JoószBelum ada peringkat
- Strahlenfolter Stalking TI Microchip Implants Mind Control and Cybernetics Naturodoc ComDokumen3 halamanStrahlenfolter Stalking TI Microchip Implants Mind Control and Cybernetics Naturodoc ComGeneration Generation100% (1)
- Strahlenfolter Brain and Satellite Surveillance RNM and EblDokumen31 halamanStrahlenfolter Brain and Satellite Surveillance RNM and EblProjekt_-stop-tortureBelum ada peringkat
- Strahlenfolter Stalking - TI - V2K - Eleanor WhiteDokumen3 halamanStrahlenfolter Stalking - TI - V2K - Eleanor WhiteHans-Georg-JakobsonBelum ada peringkat
- EMR Australian Senate Evidence 8 9 2000Dokumen85 halamanEMR Australian Senate Evidence 8 9 2000Julian HadlowBelum ada peringkat
- Antenna Basics PDFDokumen82 halamanAntenna Basics PDFSabbir AhmedBelum ada peringkat
- Ares Mission GuideDokumen17 halamanAres Mission GuideAnonymous Hnv6u54HBelum ada peringkat
- LUTEC AUSTRALIA PTY LTD Displays Prototypes That Amplifying Electricity by 5 TimesDokumen1 halamanLUTEC AUSTRALIA PTY LTD Displays Prototypes That Amplifying Electricity by 5 TimesyodifoyorBelum ada peringkat
- Intra-Body Nano-Network - Brief Summary by Mik AndersenDokumen24 halamanIntra-Body Nano-Network - Brief Summary by Mik AndersenGuilherme UnityBelum ada peringkat
- 20201213-PRESS RELEASE MR G. H. Schorel-Hlavka O.W.B. ISSUE - The World Wide 'White' Colour Revolution We Have To Have-Suppl 1Dokumen14 halaman20201213-PRESS RELEASE MR G. H. Schorel-Hlavka O.W.B. ISSUE - The World Wide 'White' Colour Revolution We Have To Have-Suppl 1Gerrit Hendrik Schorel-HlavkaBelum ada peringkat
- Electromagnetic Waves: By: I Nyoman S. (X-8/09) Raka Pandam G. (X-8/21)Dokumen11 halamanElectromagnetic Waves: By: I Nyoman S. (X-8/09) Raka Pandam G. (X-8/21)Nyoman SuryadinataBelum ada peringkat
- Strahlenfolter Stalking - TI - Robert O. Butner - Account From Mr. Joseph HohlmanDokumen16 halamanStrahlenfolter Stalking - TI - Robert O. Butner - Account From Mr. Joseph HohlmanHans-Werner-Gaertner100% (1)
- Strahlenfolter - TI - V2K - Electromagnetic Weapons and Human Rights at The 5th Symposium - Legalmerandering - Wordpress - Com - 2012Dokumen19 halamanStrahlenfolter - TI - V2K - Electromagnetic Weapons and Human Rights at The 5th Symposium - Legalmerandering - Wordpress - Com - 2012Fred_Blanke100% (1)
- Strahlenfolter Stalking - TI - What Is Electronic Harassment - Laser Harassment Devices - What Can Be Done To Protect - BugsweepsDokumen6 halamanStrahlenfolter Stalking - TI - What Is Electronic Harassment - Laser Harassment Devices - What Can Be Done To Protect - BugsweepsKurt-SchneiderBelum ada peringkat
- RNM User Kajal Kanti Dey's Photo & Tortured PhotoDokumen11 halamanRNM User Kajal Kanti Dey's Photo & Tortured PhotoKunalBelum ada peringkat
- Chief Commissioner of Victoria Police SubmissionDokumen43 halamanChief Commissioner of Victoria Police SubmissionMathewDunckleyBelum ada peringkat
- IMDDokumen111 halamanIMDTwintu VinishBelum ada peringkat
- Distracted Masses Vol. 1 Issue 2Dokumen60 halamanDistracted Masses Vol. 1 Issue 2Distracted Masses100% (2)
- Strahlenfolter - TI - How To Detect Electronic Harassment Easy - Targeted Individuals - YoutubeDokumen44 halamanStrahlenfolter - TI - How To Detect Electronic Harassment Easy - Targeted Individuals - YoutubeTimo_KaehlkeBelum ada peringkat
- 20211014-Mr G. H. Schorel-Hlavka O.W.B. To R Kershaw Chief Commissioner of The Australian Federal Police-COMPLAINT-Suppl-18-Arrest Them NowDokumen48 halaman20211014-Mr G. H. Schorel-Hlavka O.W.B. To R Kershaw Chief Commissioner of The Australian Federal Police-COMPLAINT-Suppl-18-Arrest Them NowGerrit Hendrik Schorel-Hlavka100% (1)
- 20210813-Mr G. H. Schorel-Hlavka O.W.B. To Reece Kershaw Chief Commissioner of The Australian Federal Police-COMPLAINT-Suppl-06Dokumen38 halaman20210813-Mr G. H. Schorel-Hlavka O.W.B. To Reece Kershaw Chief Commissioner of The Australian Federal Police-COMPLAINT-Suppl-06Gerrit Hendrik Schorel-HlavkaBelum ada peringkat
- Strahlenfolter Stalking - TI - Bibliotecapleyades - Net - Psychotronic Weapons - Brain Manipulation From A DistanceDokumen5 halamanStrahlenfolter Stalking - TI - Bibliotecapleyades - Net - Psychotronic Weapons - Brain Manipulation From A DistanceHans-Georg-JakobsonBelum ada peringkat
- The Hidden Dangers of Cell Phone Radiation Life Extension 2007 Aug 11ppDokumen11 halamanThe Hidden Dangers of Cell Phone Radiation Life Extension 2007 Aug 11ppMarium ShaikhBelum ada peringkat
- Physician Office LaboratoriesDokumen22 halamanPhysician Office LaboratoriesBrenda Dwi AnandhittaBelum ada peringkat
- RfidDokumen3 halamanRfidRangaprasad NallapaneniBelum ada peringkat
- Is Biochip The Mark of The Beast?Dokumen15 halamanIs Biochip The Mark of The Beast?Milmore BrachoBelum ada peringkat
- 20220419-Mr G. H. Schorel-Hlavka O.W.B. To MR Greg Hunt Minister For HealthDokumen6 halaman20220419-Mr G. H. Schorel-Hlavka O.W.B. To MR Greg Hunt Minister For HealthGerrit Hendrik Schorel-HlavkaBelum ada peringkat
- Cheryl DocumentDokumen53 halamanCheryl DocumentCINDAMOURBelum ada peringkat
- Strahlenfolter - Effects of Infra Sound On People - The Sonic Weapon - Electronic HarassmentDokumen5 halamanStrahlenfolter - Effects of Infra Sound On People - The Sonic Weapon - Electronic Harassmentnwo-mengele-doctorsBelum ada peringkat
- Strahlenfolter - Electronic Harassment - Neural Implants - Past, Present & Future PART1Dokumen11 halamanStrahlenfolter - Electronic Harassment - Neural Implants - Past, Present & Future PART1nwo-mengele-doctorsBelum ada peringkat
- GBPPR Active Denial SystemDokumen30 halamanGBPPR Active Denial SystemRobert EckardtBelum ada peringkat
- Strahlenfolter Stalking - TI - V2K - InFORMATION For PEOPLE - Hearingvoices-Is-Voicetoskull - Com IntroToGangStalkingENDokumen69 halamanStrahlenfolter Stalking - TI - V2K - InFORMATION For PEOPLE - Hearingvoices-Is-Voicetoskull - Com IntroToGangStalkingENHans-Georg-JakobsonBelum ada peringkat
- Strahlenfolter - Chip Implants Already Here - Electronic HarassmentDokumen10 halamanStrahlenfolter - Chip Implants Already Here - Electronic Harassmentnwo-mengele-doctorsBelum ada peringkat
- Why Our World Is ElectropollutedDokumen3 halamanWhy Our World Is ElectropollutedMariana AmbrosieBelum ada peringkat
- In Tell I Pedia MkultraDokumen17 halamanIn Tell I Pedia Mkultrabari jariBelum ada peringkat
- Electronic Torture - JeffPolachek - Study of Bio Ethical Issues - Mind Control Victim TestimonyDokumen14 halamanElectronic Torture - JeffPolachek - Study of Bio Ethical Issues - Mind Control Victim Testimonystop-organized-crimeBelum ada peringkat
- Mind Reading PhonesDokumen5 halamanMind Reading PhonesSiva SankarBelum ada peringkat
- Team Name: Amir Syazwan B. IbrahimDokumen9 halamanTeam Name: Amir Syazwan B. IbrahimAnas SafwanBelum ada peringkat
- Nationalreport PDFDokumen13 halamanNationalreport PDFRichard BrownBelum ada peringkat
- Strahlenfolter Stalking - TI - V2K - Movies - Gangstalking - Electronic Harassment - Voice To Skull - Implants - Hearingvoices-Is-VoicetoskullDokumen5 halamanStrahlenfolter Stalking - TI - V2K - Movies - Gangstalking - Electronic Harassment - Voice To Skull - Implants - Hearingvoices-Is-VoicetoskullHans-Georg-JakobsonBelum ada peringkat
- Bio-Electromagnetic Weapons - Open Letter From Barrie Trower - 2010Dokumen9 halamanBio-Electromagnetic Weapons - Open Letter From Barrie Trower - 2010Andreas_PietrzakBelum ada peringkat
- Nanotech BadDokumen106 halamanNanotech BadMason OwenBelum ada peringkat
- What Is The Biochip Technology - Www-Av1611-OrgDokumen17 halamanWhat Is The Biochip Technology - Www-Av1611-OrgStop-Torture-Now100% (1)
- Mind Wars ArtDokumen3 halamanMind Wars ArtBeth Book ReviewBelum ada peringkat
- Tim Rifat - Defeating Radio Based Mind Control SystemsDokumen2 halamanTim Rifat - Defeating Radio Based Mind Control SystemsGary Beaver100% (1)
- Beyond Terror: A Battered Wife on Trial for the Alleged Murder of Her HusbandDari EverandBeyond Terror: A Battered Wife on Trial for the Alleged Murder of Her HusbandBelum ada peringkat
- Mga Orasyon-7 The Ten Names of GodDokumen1 halamanMga Orasyon-7 The Ten Names of GodRed PhoenixBelum ada peringkat
- EmethDokumen8 halamanEmethRed Phoenix50% (2)
- Concealed Carry Magazine Your BestDokumen18 halamanConcealed Carry Magazine Your BestRed PhoenixBelum ada peringkat
- New Microsoft Word DocumentDokumen2 halamanNew Microsoft Word DocumentRed PhoenixBelum ada peringkat
- BRANDNEW Ranging NetLambat Made in JapanDokumen1 halamanBRANDNEW Ranging NetLambat Made in JapanRed PhoenixBelum ada peringkat
- 90 DemonsDokumen1 halaman90 DemonsRed PhoenixBelum ada peringkat
- Handloads 38 SuperDokumen19 halamanHandloads 38 SuperRed PhoenixBelum ada peringkat
- Cocker's Lunar Horoscope-Arturo de CastroDokumen2 halamanCocker's Lunar Horoscope-Arturo de CastroRed Phoenix94% (16)
- Signal KrusDokumen1 halamanSignal KrusRed PhoenixBelum ada peringkat
- The 7 Deadly MistakesDokumen35 halamanThe 7 Deadly MistakesRed PhoenixBelum ada peringkat
- The ART of COCKFIGHTING A Game of A Million Thrills by Arturo M. de CastroDokumen10 halamanThe ART of COCKFIGHTING A Game of A Million Thrills by Arturo M. de CastroRed Phoenix0% (1)
- 2014 TrijiconCatalogDokumen67 halaman2014 TrijiconCatalogRed Phoenix100% (1)
- Solutions Used For PoultryDokumen6 halamanSolutions Used For PoultryRed PhoenixBelum ada peringkat
- Vac BreedDokumen1 halamanVac BreedRed PhoenixBelum ada peringkat
- Cobb Vaccination Procedure Guide EnglishDokumen38 halamanCobb Vaccination Procedure Guide EnglishRed PhoenixBelum ada peringkat
- Corporation Code of The PhilippinesDokumen64 halamanCorporation Code of The PhilippinesChin TecsonBelum ada peringkat
- Cards As Weapons - Ricky Jay (1977)Dokumen135 halamanCards As Weapons - Ricky Jay (1977)Red Phoenix100% (4)
- Combat Archery - A Manual For Western Archers - Sir Jon Fitz-Rauf PDFDokumen30 halamanCombat Archery - A Manual For Western Archers - Sir Jon Fitz-Rauf PDFabelincoln1234Belum ada peringkat
- Comparative Analysis Between Police BatonsDokumen11 halamanComparative Analysis Between Police BatonsRed PhoenixBelum ada peringkat
- Toyota Cars PriceDokumen5 halamanToyota Cars PriceBdSulianoBelum ada peringkat
- Study GuideDokumen398 halamanStudy GuideVo HaianhBelum ada peringkat
- 5 Vocales - Sator KoronadosDokumen182 halaman5 Vocales - Sator KoronadosRed Phoenix93% (44)
- By Austin H. PhelpsDokumen4 halamanBy Austin H. PhelpsRichard TongueBelum ada peringkat
- Abulafia Cooper Messianic ConsciousnessDokumen21 halamanAbulafia Cooper Messianic ConsciousnessRed Phoenix100% (1)
- IPP 2012 - Investing in PhilippinesDokumen68 halamanIPP 2012 - Investing in Philippinesgsg5manBelum ada peringkat
- Amulets Charms TalismansDokumen118 halamanAmulets Charms TalismansRed PhoenixBelum ada peringkat
- GrimoiresDokumen11 halamanGrimoiresRed Phoenix100% (4)
- How To Begin and Survive A Commercial Gamebird Farm: "Those Who Want To Make Money Raising Gamebirds"Dokumen33 halamanHow To Begin and Survive A Commercial Gamebird Farm: "Those Who Want To Make Money Raising Gamebirds"laboraetoraBelum ada peringkat
- Inner Smile MeditationDokumen2 halamanInner Smile MeditationJox Ogris100% (1)
- Protozoan Fecal SmearDokumen17 halamanProtozoan Fecal SmearLeigh Ann TanpoBelum ada peringkat
- Greek Gods and GoddessesDokumen3 halamanGreek Gods and GoddessesKevin Macabanti100% (1)
- Scooby-Doo and The Haunted Doghouse-1Dokumen24 halamanScooby-Doo and The Haunted Doghouse-1عبد الرحمن100% (6)
- Smoking Times Temperatures Chart 2018Dokumen18 halamanSmoking Times Temperatures Chart 2018Jose JaramilloBelum ada peringkat
- Detailed Lesson Plan Music 1Dokumen6 halamanDetailed Lesson Plan Music 1Michelle Dang-iw100% (1)
- Reading Materials EnglishDokumen92 halamanReading Materials EnglishMharla JadeBelum ada peringkat
- Candor MenusDokumen4 halamanCandor MenusEaterSDBelum ada peringkat
- Laurel Park RetrospectoDokumen10 halamanLaurel Park RetrospectomichaelBelum ada peringkat
- Head and NeckDokumen11 halamanHead and NeckdrsamnBelum ada peringkat
- Ras Nsi EncounterDokumen3 halamanRas Nsi EncounterDanesh SurendranBelum ada peringkat
- The Adaptive Immune System - An OverviewDokumen48 halamanThe Adaptive Immune System - An OverviewdrkameshBelum ada peringkat
- Testicular and Scrotal DisordersDokumen127 halamanTesticular and Scrotal DisordersJean Fatima100% (1)
- Where The Red Fern Grows ReportDokumen3 halamanWhere The Red Fern Grows ReportDivine TrinitySchoolBelum ada peringkat
- 2nd Grade Journey's Unit 1 Week3 Day 1 Animal TraitsDokumen49 halaman2nd Grade Journey's Unit 1 Week3 Day 1 Animal TraitsDalia ElgamalBelum ada peringkat
- How The Elephant Got Its Big Ears by Emilee, Shelby, Terr'eDokumen7 halamanHow The Elephant Got Its Big Ears by Emilee, Shelby, Terr'eManuel LopezBelum ada peringkat
- Barbarians of Lemuria - Ancient Animals - Pdfbarbarians of Lemuria - Ancient AnimalsDokumen9 halamanBarbarians of Lemuria - Ancient Animals - Pdfbarbarians of Lemuria - Ancient Animalsgevrin100% (1)
- AntelmintikDokumen17 halamanAntelmintikRama ArdianaBelum ada peringkat
- What Is Human Body Tissue PDFDokumen3 halamanWhat Is Human Body Tissue PDFEng Abdulahi Haji100% (1)
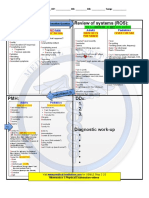
- CS Blue Sheet Mnemonics - USMLE Step 2 CS - WWW - MedicalDokumen1 halamanCS Blue Sheet Mnemonics - USMLE Step 2 CS - WWW - MedicalMaya Seegers100% (1)
- King Marangle v1.0Dokumen21 halamanKing Marangle v1.0Shawn IsaacBelum ada peringkat
- Cabbages and Cauliflowers:: James J. H. GregoryDokumen47 halamanCabbages and Cauliflowers:: James J. H. GregoryGutenberg.org100% (1)
- Script of Jungle Book PDFDokumen48 halamanScript of Jungle Book PDFHilla ManeckjiBelum ada peringkat
- Candle MagicDokumen38 halamanCandle MagicKathy Brannon Green75% (4)
- The Philippine Red CrossDokumen3 halamanThe Philippine Red CrossKeith Gretchen Lumibao CorumBelum ada peringkat
- Swinggcat - Real World Seduction 2.0Dokumen18 halamanSwinggcat - Real World Seduction 2.0wingman62567% (3)
- British Senior Section 2020-2021 Grade Igcse Anis/Premodel (E-Assessment)Dokumen12 halamanBritish Senior Section 2020-2021 Grade Igcse Anis/Premodel (E-Assessment)Khadija mBelum ada peringkat
- English Grammer PDFDokumen176 halamanEnglish Grammer PDFDrpranav SaraswatBelum ada peringkat
- Anthony D.W., Brown D.R. - Eneolithic Horse Exploitation in The Eurasian Steppes - Diet, Ritual and RidingDokumen12 halamanAnthony D.W., Brown D.R. - Eneolithic Horse Exploitation in The Eurasian Steppes - Diet, Ritual and RidingOri PerugginiBelum ada peringkat
- A Detailed Lesson Plan in English 4 For Final DemonstrationDokumen10 halamanA Detailed Lesson Plan in English 4 For Final DemonstrationHezelkiah KitaneBelum ada peringkat