Anda mungkin juga menyukai
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Terence McKenna - New Maps of Hyper SpaceDokumen10 halamanTerence McKenna - New Maps of Hyper SpaceZero One100% (2)
- (Barnardos Free Docs.) PubscatalogueDokumen12 halaman(Barnardos Free Docs.) PubscatalogueinnocentbystanderBelum ada peringkat
- The Science of ExtraterrestrialsDokumen400 halamanThe Science of Extraterrestrialsinnocentbystander100% (1)
- (Barnardos Free Docs.) Cognitive Behaviour Therapy For Behavioural Problems and Conduct Disorder in Pre-Adolescence-2Dokumen12 halaman(Barnardos Free Docs.) Cognitive Behaviour Therapy For Behavioural Problems and Conduct Disorder in Pre-Adolescence-2innocentbystanderBelum ada peringkat
- (Barnardos Free Docs.) Poverty Briefing NiDokumen8 halaman(Barnardos Free Docs.) Poverty Briefing NiinnocentbystanderBelum ada peringkat
- (Barnardos Free Docs.) Bouncing Back Resilience March09Dokumen20 halaman(Barnardos Free Docs.) Bouncing Back Resilience March09innocentbystanderBelum ada peringkat
- (Barnardos Free Docs.) It Doesn T Happen Here Full Report 8878 1Dokumen68 halaman(Barnardos Free Docs.) It Doesn T Happen Here Full Report 8878 1innocentbystanderBelum ada peringkat
- God Wants You DeadDokumen358 halamanGod Wants You Deadaadnk93% (14)
- Harmonic Resonance: DR W NelsonDokumen5 halamanHarmonic Resonance: DR W Nelsoninnocentbystander100% (1)
- Burger Boy Sporty GirlDokumen64 halamanBurger Boy Sporty GirlRoshni MahapatraBelum ada peringkat
- The Anti Terrorist Playing To WinDokumen6 halamanThe Anti Terrorist Playing To WininnocentbystanderBelum ada peringkat
- Notice To World Court On Breach of Trust Final-01Dokumen5 halamanNotice To World Court On Breach of Trust Final-01innocentbystander100% (1)
- The Nazis Go Underground - Curtis Reiss 1944Dokumen113 halamanThe Nazis Go Underground - Curtis Reiss 1944Amy Sasser100% (3)
- The Bodhisattva Way of LifeDokumen13 halamanThe Bodhisattva Way of LifeinnocentbystanderBelum ada peringkat
- The Anti Terrorist On The Freeman-Strawman-ManDokumen7 halamanThe Anti Terrorist On The Freeman-Strawman-Maninnocentbystander100% (1)
- The Anti Terrorist On Vaccines Merck and GardasilDokumen6 halamanThe Anti Terrorist On Vaccines Merck and GardasilinnocentbystanderBelum ada peringkat
- The Anti Terrorist Playing To WinDokumen6 halamanThe Anti Terrorist Playing To WininnocentbystanderBelum ada peringkat
- The Campaign For The New TimeDokumen26 halamanThe Campaign For The New TimeinnocentbystanderBelum ada peringkat
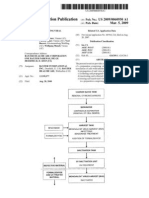
- Baxter H1N1 Vaccine Patent ApplicationDokumen10 halamanBaxter H1N1 Vaccine Patent ApplicationUSWGO Brian D. Hill100% (5)
- Thirteen Moons and The Culture of Peace - Law ofDokumen19 halamanThirteen Moons and The Culture of Peace - Law ofinnocentbystanderBelum ada peringkat
- Energy Factored by Time ArtDokumen16 halamanEnergy Factored by Time Artinnocentbystander100% (1)
- Part One of Seven On The Law of Time PartDokumen12 halamanPart One of Seven On The Law of Time PartGeCee100% (2)
- War Central Planning Corporations Schroder SchechterDokumen79 halamanWar Central Planning Corporations Schroder SchechterVen GeanciaBelum ada peringkat
- Holistic LearningDokumen27 halamanHolistic LearningLe Chu100% (14)
- Smelyakov Auric Time 2012Dokumen64 halamanSmelyakov Auric Time 2012Chad Ashley VandenbergBelum ada peringkat
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Nursing Job MotivationDokumen10 halamanNursing Job MotivationJosephine FloresBelum ada peringkat
- Forensic Psychology 5Th Edition Joanna Pozzulo Full ChapterDokumen67 halamanForensic Psychology 5Th Edition Joanna Pozzulo Full Chapterjessica.taylor655100% (7)
- 07-18-11 Montgomery County VA Jail Booking Info (Photos)Dokumen20 halaman07-18-11 Montgomery County VA Jail Booking Info (Photos)ProgressAndMainBelum ada peringkat
- MigrationDokumen327 halamanMigrationevamcbrown100% (1)
- Best Practice in Respectful Relationships Education Projects For Young People Aged 10 To 24 Years: Literature Review For Women's Health West's You, Me and Us ProjectDokumen90 halamanBest Practice in Respectful Relationships Education Projects For Young People Aged 10 To 24 Years: Literature Review For Women's Health West's You, Me and Us ProjectWomen's Health WestBelum ada peringkat
- Impact Report 2020 - March For Our LivesDokumen19 halamanImpact Report 2020 - March For Our LivesMarch For Our LivesBelum ada peringkat
- Gender EqualityDokumen16 halamanGender EqualityJapheth David (diplomat)Belum ada peringkat
- Dissertation Synopsis by UjjwalM 500076627Dokumen10 halamanDissertation Synopsis by UjjwalM 500076627Ujjwal MauryaBelum ada peringkat
- NESoHR Revives Reporting, Highlights Collective RightsDokumen9 halamanNESoHR Revives Reporting, Highlights Collective RightsThavamBelum ada peringkat
- 79 - People of The Philippines Vs Roger Ringor Umawid - Janica - 7th CaseDokumen1 halaman79 - People of The Philippines Vs Roger Ringor Umawid - Janica - 7th CaseJanica DivinagraciaBelum ada peringkat
- Political Dynasties in The PhilippinesDokumen5 halamanPolitical Dynasties in The PhilippinesmoneybymachinesBelum ada peringkat
- Letter of TransmittalDokumen11 halamanLetter of Transmittalapi-253878157Belum ada peringkat
- Antonelli e Hunt - Design and Violence-PreviewDokumen27 halamanAntonelli e Hunt - Design and Violence-PreviewAndrea Facchetti100% (1)
- 1-s2.0-S0305750X17300542 - VerDokumen20 halaman1-s2.0-S0305750X17300542 - VerNina GarfoBelum ada peringkat
- Child Abuse and The Recent Trends in Bangladesh (Study)Dokumen9 halamanChild Abuse and The Recent Trends in Bangladesh (Study)takit mallikBelum ada peringkat
- The Response To Gender-Based Violence in Eastern Europe and Central Asia - Mod-Yyyy-Mod-Mm-Mod-DdDokumen3 halamanThe Response To Gender-Based Violence in Eastern Europe and Central Asia - Mod-Yyyy-Mod-Mm-Mod-DdAndreaBelum ada peringkat
- Mexican MurdersDokumen9 halamanMexican MurdersFabiola RosalesBelum ada peringkat
- The Oxford Handbook of Criminology. (2023)Dokumen1.198 halamanThe Oxford Handbook of Criminology. (2023)Michela PirvuBelum ada peringkat
- Radio Script For Drug and Substance Abuse (Level 3) : Host: DJ AngelDokumen18 halamanRadio Script For Drug and Substance Abuse (Level 3) : Host: DJ AngelCjay LagdaanBelum ada peringkat
- Assault Charges in South Africa - Google SearchDokumen1 halamanAssault Charges in South Africa - Google SearchNathaniel MasangoBelum ada peringkat
- FOP Declaration of No ConfidenceDokumen1 halamanFOP Declaration of No ConfidenceKUTV 2NewsBelum ada peringkat
- Maam Dodie ResearchDokumen55 halamanMaam Dodie ResearchKlaris ReyesBelum ada peringkat
- CI MCQ FORMATTED 214 QuestionsDokumen34 halamanCI MCQ FORMATTED 214 QuestionsmanavBelum ada peringkat
- Gender Analysis Framework - CAREDokumen35 halamanGender Analysis Framework - CAREguru9anand100% (1)
- Gender Sensitization and Social ActionDokumen56 halamanGender Sensitization and Social ActionJoanne Rose Belle ValeBelum ada peringkat
- Strahlenfolter Stalking - TI - Targeted Individuals - Gang Stalking-Part 1 - Back To The RootsDokumen4 halamanStrahlenfolter Stalking - TI - Targeted Individuals - Gang Stalking-Part 1 - Back To The RootsOlaf-SchmidkeBelum ada peringkat
- ICPH Brief at Angled Web Homeless Family Sub Populations and Their Overlapping NeedsDokumen7 halamanICPH Brief at Angled Web Homeless Family Sub Populations and Their Overlapping NeedsMaria Cristina Schrum-HerreraBelum ada peringkat
- Workplace Violence Case StudyDokumen2 halamanWorkplace Violence Case StudyGelan OmarBelum ada peringkat
- ISEC Code of Conduct v2-1Dokumen4 halamanISEC Code of Conduct v2-1Garo KhatcherianBelum ada peringkat
- Crimes Against The Person: Bodily InjuryDokumen7 halamanCrimes Against The Person: Bodily InjuryRodney UlyateBelum ada peringkat