Anda mungkin juga menyukai
- MicrobesDokumen12 halamanMicrobesDiMa MarshBelum ada peringkat
- Herbal Drug InteractionsDokumen3 halamanHerbal Drug InteractionsFaradina Zulaili Ifa EvendyBelum ada peringkat
- Drug Side EffectsDokumen2 halamanDrug Side EffectsAngelic khanBelum ada peringkat
- Review Handouts For Medical Pharmacology: Terriann Crisp, PH.DDokumen28 halamanReview Handouts For Medical Pharmacology: Terriann Crisp, PH.Dmus zaharaBelum ada peringkat
- Antibiotics - Pathogen ChartDokumen3 halamanAntibiotics - Pathogen ChartYanling LiBelum ada peringkat
- Treatment of Chronic Heart FailureDokumen2 halamanTreatment of Chronic Heart FailureShannon RamsumairBelum ada peringkat
- ChartDokumen5 halamanChartWesley CooperBelum ada peringkat
- Pharmacology Drug ChartDokumen50 halamanPharmacology Drug ChartEssentialForLivingBelum ada peringkat
- Abx FinalDokumen3 halamanAbx Finalyanks1120Belum ada peringkat
- A New Way of Mnemonics - Hypertension-cough-asthma-NSAID - WMDokumen26 halamanA New Way of Mnemonics - Hypertension-cough-asthma-NSAID - WMKartik Mendiratta100% (1)
- Pain and Inflammation Med ChartsDokumen4 halamanPain and Inflammation Med Chartssurviving nursing school100% (1)
- MicrobialsDokumen5 halamanMicrobialsMARIEMIL FOLLOSOBelum ada peringkat
- Lecture 29 30 Thyroid TherapeuticsDokumen3 halamanLecture 29 30 Thyroid TherapeuticsAhmed MashalyBelum ada peringkat
- Respiratory System: Antiasthmatic Drugs Cardiac GlycosidesDokumen4 halamanRespiratory System: Antiasthmatic Drugs Cardiac GlycosidesNurse HoomanBelum ada peringkat
- MS2 USMLE Pharm ReviewDokumen25 halamanMS2 USMLE Pharm ReviewAnna ArtyBelum ada peringkat
- Pharma ChartsDokumen33 halamanPharma ChartsNooreen Hussain100% (1)
- Fungi Gram Positive Bacteria Viruses: Non-Tuberculous MycobacteriaDokumen1 halamanFungi Gram Positive Bacteria Viruses: Non-Tuberculous MycobacteriaImperium503Belum ada peringkat
- Drugs Acting On The AnsDokumen57 halamanDrugs Acting On The AnsAnonymous iG0DCOfBelum ada peringkat
- Micro Chart #3 - Italics OnlyDokumen27 halamanMicro Chart #3 - Italics Onlyapi-26938624100% (1)
- Journal Reading EMPEROR-ReducedDokumen21 halamanJournal Reading EMPEROR-ReducedLolii Con Harhazyuku100% (1)
- Cardiovascular Complications of Antipsychotic MedicationsDokumen3 halamanCardiovascular Complications of Antipsychotic MedicationsAakash ShahBelum ada peringkat
- Look Under Drugs Affecting Nutritional and Metbolic FunctionDokumen1 halamanLook Under Drugs Affecting Nutritional and Metbolic FunctionChrissieBelum ada peringkat
- Hand Out AntibioticsDokumen13 halamanHand Out AntibioticsMinhwa KimBelum ada peringkat
- PCOL Maps PDFDokumen11 halamanPCOL Maps PDFZinc YuloBelum ada peringkat
- Northern Ireland Management of Infection Guidelines For Primary and Community Care 2016Dokumen48 halamanNorthern Ireland Management of Infection Guidelines For Primary and Community Care 2016dreneavalentinstefanBelum ada peringkat
- Cheat Sheet For CancerDokumen4 halamanCheat Sheet For CancerEffie Cloe Marie BitengBelum ada peringkat
- Valvular Heart DiseaseDokumen4 halamanValvular Heart DiseaseAfif Al BaalbakiBelum ada peringkat
- Mu 002Dokumen10 halamanMu 002chandanBelum ada peringkat
- Pharm Drugs + Classes (All)Dokumen28 halamanPharm Drugs + Classes (All)Tom WuBelum ada peringkat
- OTC Exam 2 Study GuideDokumen32 halamanOTC Exam 2 Study GuideDave WinBelum ada peringkat
- Drugs Acting On The Gastrointestinal TractDokumen27 halamanDrugs Acting On The Gastrointestinal TractJames PerianayagamBelum ada peringkat
- Anti Infective Drug ChartDokumen1 halamanAnti Infective Drug ChartJessica100% (1)
- Onco PharmacologyDokumen9 halamanOnco Pharmacologyarn0ld21Belum ada peringkat
- Antimicrobial ReviewDokumen57 halamanAntimicrobial Reviewemiliow_1Belum ada peringkat
- Mechanism of Action For Each Class of AntiDokumen146 halamanMechanism of Action For Each Class of AntiReynaldo RiveraBelum ada peringkat
- NANDA DX NI, NODokumen165 halamanNANDA DX NI, NOKerry Brown100% (1)
- Psychiatry Pharmacology J. Psychiatry' AntidepressantsDokumen9 halamanPsychiatry Pharmacology J. Psychiatry' AntidepressantssumithjalyBelum ada peringkat
- Antibiotic Chart FinalDokumen1 halamanAntibiotic Chart FinalJosh GardnerBelum ada peringkat
- Prefix Suffix MnemonicsDokumen5 halamanPrefix Suffix MnemonicsPj MontecilloBelum ada peringkat
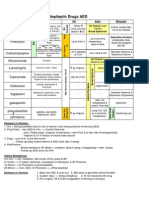
- Antiepileptic Drugs AED: D' DI Disadv SE AdvDokumen1 halamanAntiepileptic Drugs AED: D' DI Disadv SE Advrayooona88Belum ada peringkat
- Pharma CollectionDokumen40 halamanPharma CollectionMuhd Nico DariyantoBelum ada peringkat
- Histamine, Serotonin and Ergot AlkaloidsDokumen36 halamanHistamine, Serotonin and Ergot AlkaloidsSteph Taylor Reyes Radan100% (3)
- M. Pharm Review NAPLEX32Dokumen1 halamanM. Pharm Review NAPLEX32JUSASBBelum ada peringkat
- Anti-Infectives and AntibioticsDokumen38 halamanAnti-Infectives and AntibioticsKarel Lu0% (1)
- Of Angina Pectoris. Decreased Rate of Cardiovascular Mortality and Hospitalization in Patients With Heart FailureDokumen31 halamanOf Angina Pectoris. Decreased Rate of Cardiovascular Mortality and Hospitalization in Patients With Heart Failurenaikram420Belum ada peringkat
- Cogentin - Artane - Parlodel - Akineton - Benadryl - LarodopaDokumen11 halamanCogentin - Artane - Parlodel - Akineton - Benadryl - LarodopaJoseph DavidBelum ada peringkat
- Drug Interactions: What Is An Interaction?Dokumen4 halamanDrug Interactions: What Is An Interaction?Leyla MajundaBelum ada peringkat
- Pharmacy AbbreviationsDokumen6 halamanPharmacy Abbreviationscanuckiepen100% (1)
- Antibiotics 9Dokumen11 halamanAntibiotics 9Beth Morales100% (1)
- Ultimate Pharm GuideDokumen41 halamanUltimate Pharm GuideeanguyenBelum ada peringkat
- River BlindnessDokumen5 halamanRiver BlindnessBello SakanauBelum ada peringkat
- Communicable DiseasesDokumen7 halamanCommunicable DiseasesRaisa Robelle Quicho100% (1)
- Uworld Peds MicroDokumen5 halamanUworld Peds MicroJoan ChoiBelum ada peringkat
- II. Epidemiologic Descriotion of DiseasesDokumen8 halamanII. Epidemiologic Descriotion of DiseasesChristine AlmoraBelum ada peringkat
- Communicable Diseases - AntiponaDokumen79 halamanCommunicable Diseases - AntiponaRegie de JesusBelum ada peringkat
- Typhoid FeverDokumen46 halamanTyphoid Feverdeskichinta50% (2)
- Typhoid Fever: Dr. Ahmad Fariz Malvi Zamzam Zein, SP - PD Departemen Ilmu Penyakit Dalam RSUD Waled - FK UnswagatiDokumen19 halamanTyphoid Fever: Dr. Ahmad Fariz Malvi Zamzam Zein, SP - PD Departemen Ilmu Penyakit Dalam RSUD Waled - FK UnswagatiHary SaktiawanBelum ada peringkat
- Micro Final Buzz Word CheatsheetDokumen10 halamanMicro Final Buzz Word CheatsheetThesmith FamBelum ada peringkat
- Pasteurelosis: The Disease Due ToDokumen45 halamanPasteurelosis: The Disease Due Toclarentina aristawatiBelum ada peringkat
- Acute Febrile IllnessesDokumen54 halamanAcute Febrile IllnessesfraolBelum ada peringkat
- Cluster BDokumen3 halamanCluster BMegBelum ada peringkat
- Cluster A - Personality DisordersDokumen2 halamanCluster A - Personality DisordersMegBelum ada peringkat
- Urinalysis TableDokumen9 halamanUrinalysis TableMegBelum ada peringkat
- Important Lab Values Value Normal RangeDokumen1 halamanImportant Lab Values Value Normal RangeMegBelum ada peringkat
- PHC Assignment 1Dokumen5 halamanPHC Assignment 1Florenze Laiza Donor Lucas100% (1)
- Category: Capital, Tier 2: City: Bhopal State: Madhya PradeshDokumen5 halamanCategory: Capital, Tier 2: City: Bhopal State: Madhya PradeshARSHI PARASHARBelum ada peringkat
- Allocating Hospital Resources To Improve Patient ExperienceDokumen6 halamanAllocating Hospital Resources To Improve Patient ExperienceMichael0% (1)
- Comparative Analysis of National Pandemic Influenza Preparedness Plans - 2011Dokumen64 halamanComparative Analysis of National Pandemic Influenza Preparedness Plans - 2011Mohamed WahbyBelum ada peringkat
- Key To Reading 3Dokumen2 halamanKey To Reading 3Thùy TrangBelum ada peringkat
- The Brain, PT 2 - Neuroscience and BehaviorDokumen2 halamanThe Brain, PT 2 - Neuroscience and BehaviorprtemnBelum ada peringkat
- Alprazolam: Why Is This Medicine Prescribed To You?Dokumen1 halamanAlprazolam: Why Is This Medicine Prescribed To You?Jerome GeronimoBelum ada peringkat
- Nay Lin Htike-GcDokumen16 halamanNay Lin Htike-GcAsia Shwe OhBelum ada peringkat
- Drug StudyDokumen10 halamanDrug StudybaniniycsebBelum ada peringkat
- Survey QuestionnaireDokumen2 halamanSurvey Questionnairecyrusbatayan100% (1)
- Homoeopathic Perspective of Thyroid DisordersDokumen20 halamanHomoeopathic Perspective of Thyroid DisordersSaurav AroraBelum ada peringkat
- Business Ethics and Corporate Social Responsibility: Analyze Complex Issues in CSR and Corporate GovernanceDokumen6 halamanBusiness Ethics and Corporate Social Responsibility: Analyze Complex Issues in CSR and Corporate GovernanceDime PierrowBelum ada peringkat
- Health and Welfare Committee ReportDokumen4 halamanHealth and Welfare Committee ReporttncircuitriderBelum ada peringkat
- 12 Week ProgramDokumen45 halaman12 Week ProgramCow SapiBelum ada peringkat
- Hafiz Fizalia - Acupuncture Hack - The Easiest Way To Learn Classical Theories of Acupuncture (2018) PDFDokumen66 halamanHafiz Fizalia - Acupuncture Hack - The Easiest Way To Learn Classical Theories of Acupuncture (2018) PDFkhalid Sijilmassi100% (3)
- Mustafa CV PDFDokumen22 halamanMustafa CV PDFMUSTAFA TEMEMIBelum ada peringkat
- Diabetic Foot Ulcer Assessment and Management Algorithm - 0Dokumen11 halamanDiabetic Foot Ulcer Assessment and Management Algorithm - 0Herlan BelaBelum ada peringkat
- APDSA SRC Submitssion FormDokumen2 halamanAPDSA SRC Submitssion FormDevi 吴姗姗 GunawanBelum ada peringkat
- Paper On Rag PickersDokumen11 halamanPaper On Rag PickershsrapsBelum ada peringkat
- Checklist of Requirements For Over The Counter Preparations and Household RemediesDokumen2 halamanChecklist of Requirements For Over The Counter Preparations and Household RemediesBSS100% (1)
- Effects of Child Abuse and Neglect For Children and AdolescentsDokumen15 halamanEffects of Child Abuse and Neglect For Children and AdolescentsMaggie YungBelum ada peringkat
- Professional Review Industry Route Guidance NotesDokumen10 halamanProfessional Review Industry Route Guidance NotesAnonymous TlYmhkBelum ada peringkat
- 5 Cover Letter Samples For Your Scientific ManuscriptDokumen11 halaman5 Cover Letter Samples For Your Scientific ManuscriptAlejandra J. Troncoso100% (2)
- Building Occupational Safety and Health k3 Analysis of The Work Environment and Work DisciplineDokumen10 halamanBuilding Occupational Safety and Health k3 Analysis of The Work Environment and Work Disciplineipraul167Belum ada peringkat
- Estimation of Uric Acid Levels in SerumDokumen6 halamanEstimation of Uric Acid Levels in Serumvicky_law_275% (4)
- Crane Workbox 4398Dokumen4 halamanCrane Workbox 4398hazopman100% (1)
- Clinical Practice Guidelines: High-Grade Glioma: ESMO Clinical Practice Guidelines For Diagnosis, Treatment and Follow-UpDokumen9 halamanClinical Practice Guidelines: High-Grade Glioma: ESMO Clinical Practice Guidelines For Diagnosis, Treatment and Follow-UpSiva SubramaniamBelum ada peringkat
- Jdo Vol 59 New PDFDokumen100 halamanJdo Vol 59 New PDFLex MBelum ada peringkat
- Presented by Heena KousarDokumen50 halamanPresented by Heena KousarSreejil RaveendranBelum ada peringkat
- COUNCIL DIRECTIVE 90 269 EEC On The Minimum Health and Safety Requirements For The Manual Handling of LoadsDokumen7 halamanCOUNCIL DIRECTIVE 90 269 EEC On The Minimum Health and Safety Requirements For The Manual Handling of Loadsromedic36Belum ada peringkat