Anda mungkin juga menyukai
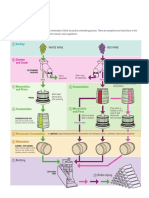
- Winemaking Booklet ProsperoDokumen44 halamanWinemaking Booklet ProsperoantonioforteseBelum ada peringkat
- Asthma Diagnosis Monitoring and Chronic Asthma Management PDF 1837687975621Dokumen39 halamanAsthma Diagnosis Monitoring and Chronic Asthma Management PDF 1837687975621hisham hussainBelum ada peringkat
- Medicine and SurgeryDokumen552 halamanMedicine and Surgeryhoneyjoy76100% (2)
- Adult Asthma Action PlanDokumen2 halamanAdult Asthma Action PlanantonioforteseBelum ada peringkat
- GINA 2019 Main Report June 2019 Wms PDFDokumen201 halamanGINA 2019 Main Report June 2019 Wms PDFAndrada PredaBelum ada peringkat
- Asthma: Allergy Asthma and Clinical Immunology November 2011Dokumen10 halamanAsthma: Allergy Asthma and Clinical Immunology November 2011Sarmad AlwardiBelum ada peringkat
- Wine GuideDokumen4 halamanWine GuidepankajkhakareBelum ada peringkat
- Doping in Sport - ReviewDokumen5 halamanDoping in Sport - ReviewantonioforteseBelum ada peringkat
- Stone Bee BiologyDokumen23 halamanStone Bee BiologyHRTOCBelum ada peringkat
- BeesInDecline PDFDokumen48 halamanBeesInDecline PDFanon_635471414Belum ada peringkat
- Nuclear Medicine: Science and Safety: Canadian Medical Association Journal October 1996Dokumen3 halamanNuclear Medicine: Science and Safety: Canadian Medical Association Journal October 1996antonioforteseBelum ada peringkat
- BeesInDecline PDFDokumen48 halamanBeesInDecline PDFanon_635471414Belum ada peringkat
- ClematisDokumen2 halamanClematisantonioforteseBelum ada peringkat
- Genitourinary UltrasoundDokumen62 halamanGenitourinary Ultrasoundantoniofortese100% (2)
- Free 12 X 8 Shed Plan - Step by Step DIYDokumen24 halamanFree 12 X 8 Shed Plan - Step by Step DIYgo2top2Belum ada peringkat
- Story of Honey WebDokumen11 halamanStory of Honey WebantonioforteseBelum ada peringkat
- The Backyard Gardener - Simple, Easy, and Beautiful Gardening With Vegetables, Herbs, and FlowersDokumen257 halamanThe Backyard Gardener - Simple, Easy, and Beautiful Gardening With Vegetables, Herbs, and Flowersantoniofortese100% (3)
- Fuchsia CareDokumen2 halamanFuchsia CareantonioforteseBelum ada peringkat
- Alyssum - LobulariaDokumen1 halamanAlyssum - LobulariaantonioforteseBelum ada peringkat
- Elastography of ThyroidDokumen8 halamanElastography of ThyroidantonioforteseBelum ada peringkat
- Growing Fuchsias in The Ground-Barbara's Way: Soil and PositionDokumen4 halamanGrowing Fuchsias in The Ground-Barbara's Way: Soil and PositionantonioforteseBelum ada peringkat
- Achillea - YarrowDokumen1 halamanAchillea - YarrowantonioforteseBelum ada peringkat
- Floral DiseasesDokumen3 halamanFloral DiseasesantonioforteseBelum ada peringkat
- Acanthus Mollis - Bears BreechesDokumen1 halamanAcanthus Mollis - Bears BreechesantonioforteseBelum ada peringkat
- DahliaDokumen2 halamanDahliaantonioforteseBelum ada peringkat
- GAZANIADokumen1 halamanGAZANIAantonioforteseBelum ada peringkat
- CoreopsisDokumen1 halamanCoreopsisantonioforteseBelum ada peringkat
- L Ily-O F-TH E-Va Lley: Featu Res ConditionsDokumen1 halamanL Ily-O F-TH E-Va Lley: Featu Res ConditionsantonioforteseBelum ada peringkat
- Ianthus Barbatus: Sweet WilliamDokumen4 halamanIanthus Barbatus: Sweet WilliamantonioforteseBelum ada peringkat
- Aurinia Saxat1Lis: Golden DustDokumen1 halamanAurinia Saxat1Lis: Golden DustantonioforteseBelum ada peringkat
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Pineapple in JohorDokumen6 halamanPineapple in JohorHaiqal AzizBelum ada peringkat
- GLP BmsDokumen18 halamanGLP BmsDr.Subhashish TripathyBelum ada peringkat
- Math 202 Syllabus-Spring18 PDFDokumen2 halamanMath 202 Syllabus-Spring18 PDFvonacoc49Belum ada peringkat
- Dialog Bahasa InggirsDokumen2 halamanDialog Bahasa InggirsKeRtha NeghaRaBelum ada peringkat
- Communication Guide: For Vita 62 Compliant VPX Power SuppliesDokumen8 halamanCommunication Guide: For Vita 62 Compliant VPX Power Suppliesk.saikumarBelum ada peringkat
- UC Lennox Serie 13 Acx Merit R-410aDokumen52 halamanUC Lennox Serie 13 Acx Merit R-410ajmurcia80Belum ada peringkat
- Intumescent Paint For Steel NZ - Coating - Co.nzDokumen8 halamanIntumescent Paint For Steel NZ - Coating - Co.nzPeter ThomsonBelum ada peringkat
- American University of BeirutDokumen21 halamanAmerican University of BeirutWomens Program AssosciationBelum ada peringkat
- Table 1 Minimum Separation DistancesDokumen123 halamanTable 1 Minimum Separation DistancesjhonBelum ada peringkat
- Government of West Bengal:: Tata Motors LTD: Abc 1 1 1 1 NA 0 NA 0Dokumen1 halamanGovernment of West Bengal:: Tata Motors LTD: Abc 1 1 1 1 NA 0 NA 0md taj khanBelum ada peringkat
- Navy Supplement To The DOD Dictionary of Military and Associated Terms, 2011Dokumen405 halamanNavy Supplement To The DOD Dictionary of Military and Associated Terms, 2011bateljupko100% (1)
- 09.tracheostomy Management by Speech Language Pathologists in SwedenDokumen12 halaman09.tracheostomy Management by Speech Language Pathologists in SwedenCarlonchaCáceresBelum ada peringkat
- Modified Phosphate and Silica Waste in Pigment PaintDokumen12 halamanModified Phosphate and Silica Waste in Pigment PaintDani M RamdhaniBelum ada peringkat
- Typical Section SC 10: Kerajaan MalaysiaDokumen1 halamanTypical Section SC 10: Kerajaan MalaysiaAisyah Atiqah KhalidBelum ada peringkat
- Hot Topic 02 Good Light Magazine 56smDokumen24 halamanHot Topic 02 Good Light Magazine 56smForos IscBelum ada peringkat
- Properties of Matter ReviewDokumen8 halamanProperties of Matter Reviewapi-290100812Belum ada peringkat
- Bahir Dar University BIT: Faculity of Mechanical and Industrial EngineeringDokumen13 halamanBahir Dar University BIT: Faculity of Mechanical and Industrial Engineeringfraol girmaBelum ada peringkat
- BS746 2014Dokumen22 halamanBS746 2014marco SimonelliBelum ada peringkat
- Mathematical Modeling of Mechanical Systems and Electrical SystemsDokumen49 halamanMathematical Modeling of Mechanical Systems and Electrical SystemsMary DunhamBelum ada peringkat
- LJ-V7080 DatasheetDokumen2 halamanLJ-V7080 DatasheetOrhan DenizliBelum ada peringkat
- Chennai To Vishakhapatnam El6Vvd: Indigo 6E-6835Dokumen3 halamanChennai To Vishakhapatnam El6Vvd: Indigo 6E-6835VENKATESH POONDRUBelum ada peringkat
- The Dry Bulk Management StandardDokumen18 halamanThe Dry Bulk Management Standardamu_more44100% (1)
- Me8072 Renewable Sources of EnergyDokumen13 halamanMe8072 Renewable Sources of EnergyNallappan Rajj ABelum ada peringkat
- Manufacuring EngineeringDokumen3 halamanManufacuring Engineeringapi-79207659Belum ada peringkat
- Michelle LeBaron, Venashri - Pillay) Conflict AcrosDokumen241 halamanMichelle LeBaron, Venashri - Pillay) Conflict AcrosBader100% (2)
- Generalized Anxiety DisorderDokumen24 halamanGeneralized Anxiety DisorderEula Angelica OcoBelum ada peringkat
- Monkeys PawDokumen4 halamanMonkeys PawKaitlin HartmanBelum ada peringkat
- Understanding Bernoulli's Principle Through Simulations PDFDokumen4 halamanUnderstanding Bernoulli's Principle Through Simulations PDFIoannis GaroufalidisBelum ada peringkat
- Final Thesis - Aris PotliopoulosDokumen94 halamanFinal Thesis - Aris PotliopoulosCristinaBelum ada peringkat
- JHS 182Dokumen137 halamanJHS 182harbhajan singhBelum ada peringkat