Anda mungkin juga menyukai
- 2016 - Association Between Vestibular and Cognitive FunctionDokumen8 halaman2016 - Association Between Vestibular and Cognitive FunctionDenise MaiaBelum ada peringkat
- Phys Ther 1998 Smithson 577 92Dokumen18 halamanPhys Ther 1998 Smithson 577 9246238148Belum ada peringkat
- Balance and Mobility Dysfunction and Falls Risk in Older People With Mild To Moderate Alzheimer DiseaseDokumen12 halamanBalance and Mobility Dysfunction and Falls Risk in Older People With Mild To Moderate Alzheimer DiseaseSintia ApriantiBelum ada peringkat
- Otago Home-Based Strength and Balance Retraining Improves Executive Functioning in Older Fallers - A Randomized Controlled Trial.Dokumen10 halamanOtago Home-Based Strength and Balance Retraining Improves Executive Functioning in Older Fallers - A Randomized Controlled Trial.Ed RibeiroBelum ada peringkat
- Son 2016Dokumen4 halamanSon 2016Zaki RiciBelum ada peringkat
- Ggi12193 PDF Jsessionid f01t02Dokumen9 halamanGgi12193 PDF Jsessionid f01t02omboBelum ada peringkat
- SPPB Short Physical Performance SCOREDokumen6 halamanSPPB Short Physical Performance SCOREruth lopezBelum ada peringkat
- Ingemar S SonDokumen10 halamanIngemar S SonViolant Verges ForesBelum ada peringkat
- Muscle Force and Range of Motion Predictors of Balance in CPDokumen21 halamanMuscle Force and Range of Motion Predictors of Balance in CPshodhgangaBelum ada peringkat
- Disability and DMDokumen15 halamanDisability and DMCelia RodriguezBelum ada peringkat
- Cardiorespiratory HOMODokumen9 halamanCardiorespiratory HOMODyah SafitriBelum ada peringkat
- Hospital Therapy Dog Walking For Adolesc Orthopedic LimitationsDokumen17 halamanHospital Therapy Dog Walking For Adolesc Orthopedic LimitationsOnte FelizBelum ada peringkat
- Genu Valgum and Flat Feet in Children With Healthy.15Dokumen7 halamanGenu Valgum and Flat Feet in Children With Healthy.15saarita lozano piedraBelum ada peringkat
- Normative Values For The Unipedal Stance Test Springer-JGPTDokumen8 halamanNormative Values For The Unipedal Stance Test Springer-JGPTblitzkrieg5891Belum ada peringkat
- Physical ActivityDokumen5 halamanPhysical ActivityshaviraBelum ada peringkat
- 431 2016 Article 2839Dokumen6 halaman431 2016 Article 2839rayalarasatitiBelum ada peringkat
- 2016 Bauer Prediction of Future Falls in A CommunityDokumen16 halaman2016 Bauer Prediction of Future Falls in A CommunityFelipe RetamalBelum ada peringkat
- Hackney 2007Dokumen19 halamanHackney 2007EmeseBelum ada peringkat
- A-The Development of Mature Gait - 1980Dokumen3 halamanA-The Development of Mature Gait - 1980Gaetano Lo BueBelum ada peringkat
- S 0035 1565915 PDFDokumen8 halamanS 0035 1565915 PDFSandu DidencuBelum ada peringkat
- Balance and Gait in The Elderly - A Contemporary Review Q1Dokumen11 halamanBalance and Gait in The Elderly - A Contemporary Review Q1MaríaPazQuitoBelum ada peringkat
- Ictus Ortesis MmiiDokumen10 halamanIctus Ortesis MmiiCeto Ust Puerto MonttBelum ada peringkat
- The Reliability and Validity of The Four Square Step Test For People With Balance Deficits Secondary To A Vestibular DisorderDokumen6 halamanThe Reliability and Validity of The Four Square Step Test For People With Balance Deficits Secondary To A Vestibular Disordergiovanni senzaterraBelum ada peringkat
- Exercise Training Program in Children and Adolescents With Cerebral PalsyDokumen7 halamanExercise Training Program in Children and Adolescents With Cerebral PalsyValentina SiegmundBelum ada peringkat
- Sensorimotor Training For BalanceDokumen7 halamanSensorimotor Training For BalanceAgatha SharmaBelum ada peringkat
- (129 136) V9N5PTDokumen8 halaman(129 136) V9N5PTAqila NurBelum ada peringkat
- NR439 W5 Reading Research Literature Form Hannah DorvilDokumen7 halamanNR439 W5 Reading Research Literature Form Hannah DorvilChris Amedjonekou100% (5)
- Physical Mobility, Physical Activity, and Obesity Among Elderly: Findings From A Large Population-Based Swedish SurveyDokumen8 halamanPhysical Mobility, Physical Activity, and Obesity Among Elderly: Findings From A Large Population-Based Swedish SurveyLiga BolaBelum ada peringkat
- Association Between A Comprehensive Movement Assesment and MetabolicallyDokumen9 halamanAssociation Between A Comprehensive Movement Assesment and MetabolicallyzunigasanBelum ada peringkat
- Beyer 2007Dokumen10 halamanBeyer 2007DR NOOR AZLIYANA AZIZANBelum ada peringkat
- 1 s2.0 S2095254615000952 MainDokumen6 halaman1 s2.0 S2095254615000952 MainwissalBelum ada peringkat
- Reliability of Gait Performance Tests in Men and Women With Hemiparesis After StrokeDokumen8 halamanReliability of Gait Performance Tests in Men and Women With Hemiparesis After StrokeKaniBelum ada peringkat
- 2193 Dsadsawqdwq1801 3 543Dokumen6 halaman2193 Dsadsawqdwq1801 3 543Sigop Elliot LBelum ada peringkat
- J Gaitpost 2019 01 005Dokumen25 halamanJ Gaitpost 2019 01 005dia putriBelum ada peringkat
- ProQuestDocuments 2017 11 11 PDFDokumen13 halamanProQuestDocuments 2017 11 11 PDFDonny HendrawanBelum ada peringkat
- Joernal 3Dokumen13 halamanJoernal 3Dyra DizhwarBelum ada peringkat
- Jurnal 10 1 JuwDokumen15 halamanJurnal 10 1 JuwvaniaBelum ada peringkat
- Effect of The Auricular Acupoint Associated With Physical Exercise in Elderly People: A Randomized Clinical TestDokumen8 halamanEffect of The Auricular Acupoint Associated With Physical Exercise in Elderly People: A Randomized Clinical TestRafael FontesBelum ada peringkat
- Timed Up and Down Stairs Validity and ReliabilityDokumen9 halamanTimed Up and Down Stairs Validity and ReliabilityAndrea B DullanoBelum ada peringkat
- Lowe 2015Dokumen9 halamanLowe 2015ﻱﺪﺢ ﺁﻏﻦﻎBelum ada peringkat
- Clinical Biomechanics: A A C C A BDokumen6 halamanClinical Biomechanics: A A C C A BJorge De Araujo RochaBelum ada peringkat
- Dafpus 11Dokumen9 halamanDafpus 11Cut MulianiBelum ada peringkat
- The Analysis of Gait in People With Down SyndromeDokumen10 halamanThe Analysis of Gait in People With Down Syndromeindah 123Belum ada peringkat
- Types of Gait Disorders ReviewDokumen12 halamanTypes of Gait Disorders ReviewkaustubhBelum ada peringkat
- Assessing PhysicalDokumen11 halamanAssessing PhysicaljuanlofishBelum ada peringkat
- s00586 010 1543 2Dokumen11 halamans00586 010 1543 2mohamed hazemBelum ada peringkat
- Ymj 59 317Dokumen8 halamanYmj 59 317ItaloLozanoPalominoBelum ada peringkat
- Aging, Muscle Activity, and Balance Control: Physiologic Changes Associated With Balance ImpairmentDokumen8 halamanAging, Muscle Activity, and Balance Control: Physiologic Changes Associated With Balance ImpairmentFrancisco Vicent PachecoBelum ada peringkat
- Relationship of Body Fat and Cardiorespiratory Fitness With Cardiovascular Risk in Chinese ChildrenDokumen5 halamanRelationship of Body Fat and Cardiorespiratory Fitness With Cardiovascular Risk in Chinese ChildrenArya KusumaBelum ada peringkat
- Diferenças de Gênero Nos Padrões de Atividade Física Entre Idosos Que CaemDokumen7 halamanDiferenças de Gênero Nos Padrões de Atividade Física Entre Idosos Que CaemLuise Lara GosuenBelum ada peringkat
- Jenna e and Nikki R Ebp Final Alt With Accepted ChangesDokumen14 halamanJenna e and Nikki R Ebp Final Alt With Accepted Changesapi-435782808Belum ada peringkat
- Effect of Square Stepping Exercise Versus Swiss Ball Exercise On Balance in Institutionalized Elderly PopulationDokumen6 halamanEffect of Square Stepping Exercise Versus Swiss Ball Exercise On Balance in Institutionalized Elderly Populationastrinila fauziBelum ada peringkat
- ผลงานวิจัย Wp RbDokumen7 halamanผลงานวิจัย Wp RbMuhammad Ilham MaulanaBelum ada peringkat
- Loss of Olfactory Function and Nutritional Status in Vital Older Adults and Geriatric PatientsDokumen7 halamanLoss of Olfactory Function and Nutritional Status in Vital Older Adults and Geriatric PatientselenaBelum ada peringkat
- 1 s2.0 S0165587622001008 MainDokumen5 halaman1 s2.0 S0165587622001008 MaintesteiroBelum ada peringkat
- Optimizing The Combination of Oxytocin M 7872188dDokumen6 halamanOptimizing The Combination of Oxytocin M 7872188dAnggi WidyaBelum ada peringkat
- Research in Developmental DisabilitiesDokumen12 halamanResearch in Developmental DisabilitiesRun CapBelum ada peringkat
- Paterson (2010) - Gait Variability, Stride Dynamics and Falls Risk in Community Dwelling Older WomenDokumen287 halamanPaterson (2010) - Gait Variability, Stride Dynamics and Falls Risk in Community Dwelling Older Womenzineb1el1attar1sofiBelum ada peringkat
- Performance-Based Physical FunctionDokumen6 halamanPerformance-Based Physical FunctionBruna MacedoBelum ada peringkat
- Disorders of the Patellofemoral Joint: Diagnosis and ManagementDari EverandDisorders of the Patellofemoral Joint: Diagnosis and ManagementBelum ada peringkat
- Minggu Ke-5 Bulan Maret 2018Dokumen3 halamanMinggu Ke-5 Bulan Maret 2018Anang FajarBelum ada peringkat
- Referred From Orthopaedic Outpatient Clinic With Neglected Dislocation Elbow S Post Open ReductionDokumen1 halamanReferred From Orthopaedic Outpatient Clinic With Neglected Dislocation Elbow S Post Open ReductionAnang FajarBelum ada peringkat
- LifesaverDokumen14 halamanLifesaverAnang FajarBelum ada peringkat
- Af Af: Aka Aka Aka Aka Aka AkaDokumen3 halamanAf Af: Aka Aka Aka Aka Aka AkaAnang FajarBelum ada peringkat
- Referral of Medical Rehabilitation Hospital Poly Pamekasan With BellDokumen1 halamanReferral of Medical Rehabilitation Hospital Poly Pamekasan With BellAnang FajarBelum ada peringkat
- Rhs 15Dokumen8 halamanRhs 15Anang FajarBelum ada peringkat
- PHYS THER 2012 Stevens Lapsley 210 26Dokumen19 halamanPHYS THER 2012 Stevens Lapsley 210 26Anang FajarBelum ada peringkat
- Fibro 4Dokumen3 halamanFibro 4Anang FajarBelum ada peringkat
- Reproduction of Overall Spontaneous Pain Pattern by Manual Stimulation of Active Myofascial Trigger Points in Fibromyalgia PatientsDokumen7 halamanReproduction of Overall Spontaneous Pain Pattern by Manual Stimulation of Active Myofascial Trigger Points in Fibromyalgia PatientsAnang FajarBelum ada peringkat
- Rhs 15Dokumen8 halamanRhs 15Anang FajarBelum ada peringkat
- Phys Ther 2012 Ioppolo 1376 85Dokumen12 halamanPhys Ther 2012 Ioppolo 1376 85Anang FajarBelum ada peringkat
- Referral of Medical Rehabilitation Hospital Poly Pamekasan With BellDokumen1 halamanReferral of Medical Rehabilitation Hospital Poly Pamekasan With BellAnang FajarBelum ada peringkat
- Phys Ther 2012 Macedo 363 77Dokumen18 halamanPhys Ther 2012 Macedo 363 77Anang FajarBelum ada peringkat
- CH02 SampleDokumen26 halamanCH02 SampleAnang FajarBelum ada peringkat
- 13 585aDokumen2 halaman13 585aAnang FajarBelum ada peringkat
- Referred From Orthopaedic Outpatient Clinic With Neglected Dislocation Elbow S Post Open ReductionDokumen1 halamanReferred From Orthopaedic Outpatient Clinic With Neglected Dislocation Elbow S Post Open ReductionAnang FajarBelum ada peringkat
- Pre-Conditioning Exercise Techniques and Supplements to Increase Stress ToleranceDokumen24 halamanPre-Conditioning Exercise Techniques and Supplements to Increase Stress ToleranceAnang FajarBelum ada peringkat
- Cervical Root Syndrome Sc4Dokumen50 halamanCervical Root Syndrome Sc4Anang FajarBelum ada peringkat
- Rehabilitation of Overhead Shoulder InjuriesDokumen3 halamanRehabilitation of Overhead Shoulder InjuriesAnang FajarBelum ada peringkat
- Imaging Anterior Cruciate Ligament Tear - Helpful Tips Imaging Anterior Cruciate Ligament Tear - Helpful TipsDokumen5 halamanImaging Anterior Cruciate Ligament Tear - Helpful Tips Imaging Anterior Cruciate Ligament Tear - Helpful TipsAnang FajarBelum ada peringkat
- Referred From Orthopaedic Outpatient Clinic With Neglected Dislocation Elbow S Post Open ReductionDokumen1 halamanReferred From Orthopaedic Outpatient Clinic With Neglected Dislocation Elbow S Post Open ReductionAnang FajarBelum ada peringkat
- Cervical Root SyndromeDokumen48 halamanCervical Root SyndromeAnang FajarBelum ada peringkat
- Ankle Tendon InjuryDokumen7 halamanAnkle Tendon InjuryAnang FajarBelum ada peringkat
- Rehabilitation After ACL ReconstructionDokumen4 halamanRehabilitation After ACL ReconstructionAnang FajarBelum ada peringkat
- De Quervain's Tenosynovitis: By: Dr. HermilawatyDokumen35 halamanDe Quervain's Tenosynovitis: By: Dr. HermilawatyAnang FajarBelum ada peringkat
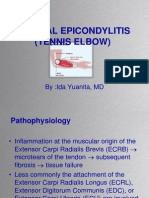
- Lateral Epicondylitis (Tennis Elbow) : By:Ida Yuanita, MDDokumen37 halamanLateral Epicondylitis (Tennis Elbow) : By:Ida Yuanita, MDAnang FajarBelum ada peringkat
- Trigger Finger TreatmentDokumen33 halamanTrigger Finger TreatmentAnang FajarBelum ada peringkat
- Biomechanics and MOI of The AnkleDokumen37 halamanBiomechanics and MOI of The AnkleAnang FajarBelum ada peringkat
- Carpal Tunnel Syndrome: by A. A. Sagung Mas CahyandariDokumen37 halamanCarpal Tunnel Syndrome: by A. A. Sagung Mas CahyandariAnang FajarBelum ada peringkat
- 016-5032-002-C - SmarTrax - Case IH STX-Steiger-Quadtrac (AccuGuide-Ready) and New Holland TJ-T90X0-T9XXX (IntelliSteer-Ready) - Installation ManualDokumen26 halaman016-5032-002-C - SmarTrax - Case IH STX-Steiger-Quadtrac (AccuGuide-Ready) and New Holland TJ-T90X0-T9XXX (IntelliSteer-Ready) - Installation ManualAndreyBelum ada peringkat
- Chapter 1: Abnormal Behavior in Historical ContextDokumen22 halamanChapter 1: Abnormal Behavior in Historical ContextEsraRamos100% (2)
- Ageism PowerpointDokumen11 halamanAgeism Powerpointapi-254132646Belum ada peringkat
- CALIS ScoringDokumen2 halamanCALIS ScoringIqbal BaryarBelum ada peringkat
- Annex C Olp On The RoadDokumen7 halamanAnnex C Olp On The RoadCabanglasanfs OLPBelum ada peringkat
- Lesson 1:: Introduction To Science, Technology and SocietyDokumen17 halamanLesson 1:: Introduction To Science, Technology and SocietyAlexis A. AguilarBelum ada peringkat
- M96SC05 Oleo StrutDokumen6 halamanM96SC05 Oleo Strutchaumont12345Belum ada peringkat
- Supplementary Feeding ProgramDokumen2 halamanSupplementary Feeding ProgramVictor Anthony CuaresmaBelum ada peringkat
- Chapter - 10 NanoshellsDokumen13 halamanChapter - 10 NanoshellskarthikBelum ada peringkat
- Bill 192: An Act To Ensure Student Health and Safety in The Classroom by Regulating Ambient Air Quality in SchoolsDokumen8 halamanBill 192: An Act To Ensure Student Health and Safety in The Classroom by Regulating Ambient Air Quality in SchoolsCtv MontrealBelum ada peringkat
- ESP Guidance For All Ships V13.7Dokumen53 halamanESP Guidance For All Ships V13.7Jayasankar GopalakrishnanBelum ada peringkat
- Soni Clinic & Pathology Center Chanda: Address:-Front of TVS AgencyDokumen1 halamanSoni Clinic & Pathology Center Chanda: Address:-Front of TVS AgencyVishalBelum ada peringkat
- BSN-2D 1st Semester ScheduleDokumen2 halamanBSN-2D 1st Semester ScheduleReyjan ApolonioBelum ada peringkat
- Manual Murray 20Dokumen28 halamanManual Murray 20freebanker777741Belum ada peringkat
- Section III - Topic 3Dokumen7 halamanSection III - Topic 3KARINE HOVSEPYANBelum ada peringkat
- Prof Educ 2: Foundation of Special and Inclusive EducationDokumen12 halamanProf Educ 2: Foundation of Special and Inclusive EducationNerissa Custosa BastoBelum ada peringkat
- Archives of Oral Biology 100 (2019) 42-48Dokumen7 halamanArchives of Oral Biology 100 (2019) 42-48pedro cuellar proBelum ada peringkat
- Review of Literature Review of LiteratureDokumen31 halamanReview of Literature Review of LiteratureeswariBelum ada peringkat
- Writing About Emotional Experiences As A Therapeutic Process PDFDokumen6 halamanWriting About Emotional Experiences As A Therapeutic Process PDFOscarBelum ada peringkat
- Installation TubeeeDokumen7 halamanInstallation TubeeeDini NovitrianingsihBelum ada peringkat
- Computed Tomography (CT) - BodyDokumen7 halamanComputed Tomography (CT) - Bodyfery oktoraBelum ada peringkat
- Structure Dismantling JSADokumen2 halamanStructure Dismantling JSAtnssbhaskar69% (13)
- START-HERE Ch11 LectureDokumen84 halamanSTART-HERE Ch11 LecturePraveen VootlaBelum ada peringkat
- Intermediate Alloy Steels Properties and SpecificationsDokumen15 halamanIntermediate Alloy Steels Properties and Specificationsanon_558118723100% (1)
- Asian Organized CrimeDokumen17 halamanAsian Organized CrimeMagr EscaBelum ada peringkat
- EIM GRADE 9 10 Q4 Module 1b - National Electrical Code NEC Provisions in Installing Wiring Devices - GFCI. - FinalDokumen23 halamanEIM GRADE 9 10 Q4 Module 1b - National Electrical Code NEC Provisions in Installing Wiring Devices - GFCI. - FinalTitser Ramca100% (3)
- 'S Outfits and Emergency Escape Breathing Devices (Eebd)Dokumen11 halaman'S Outfits and Emergency Escape Breathing Devices (Eebd)Thurdsuk NoinijBelum ada peringkat
- 6th Class EM All LessonsDokumen33 halaman6th Class EM All LessonsSathish PurushothamBelum ada peringkat
- Chronic Pain GuidelinesDokumen56 halamanChronic Pain GuidelinesOporadhBiggan100% (1)
- Fall ProtectionDokumen5 halamanFall ProtectionAamir AliBelum ada peringkat