Anda mungkin juga menyukai
- Ap 1 PDFDokumen7 halamanAp 1 PDFdonkeyendutBelum ada peringkat
- Wrist Sizing Hamilton PDFDokumen3 halamanWrist Sizing Hamilton PDFdonkeyendutBelum ada peringkat
- Analisa Dan Penanganan Hepatitis Kemenkes RIDokumen8 halamanAnalisa Dan Penanganan Hepatitis Kemenkes RIIzzi FekratBelum ada peringkat
- Wrist Sizing HamiltonDokumen3 halamanWrist Sizing HamiltondonkeyendutBelum ada peringkat
- Dep 1 PDFDokumen11 halamanDep 1 PDFdonkeyendutBelum ada peringkat
- Dopamin 2 PDFDokumen8 halamanDopamin 2 PDFdonkeyendutBelum ada peringkat
- Fatique and Artritis Psoriatic PDFDokumen72 halamanFatique and Artritis Psoriatic PDFdonkeyendutBelum ada peringkat
- Turgor KulitDokumen21 halamanTurgor KulitChairunisa AnggrainiBelum ada peringkat
- Tesis Lampiran 9Dokumen5 halamanTesis Lampiran 9donkeyendutBelum ada peringkat
- Looking Beyond The Monoamine Hypothesis: Johan A Den BoerDokumen9 halamanLooking Beyond The Monoamine Hypothesis: Johan A Den BoerdonkeyendutBelum ada peringkat
- ADTI SMMSE-GDS Reference Card PDFDokumen2 halamanADTI SMMSE-GDS Reference Card PDFSummer WrightBelum ada peringkat
- Depression Theory PDFDokumen2 halamanDepression Theory PDFdonkeyendutBelum ada peringkat
- Mekanisme Aksi DopaminDokumen14 halamanMekanisme Aksi DopamindonkeyendutBelum ada peringkat
- HHLDokumen7 halamanHHLdonkeyendutBelum ada peringkat
- Gold WR 06Dokumen100 halamanGold WR 06Melissa VidalesBelum ada peringkat
- Summary Sepsis ManagementDokumen60 halamanSummary Sepsis ManagementdonkeyendutBelum ada peringkat
- How To Measure Cd14Dokumen38 halamanHow To Measure Cd14donkeyendutBelum ada peringkat
- Jurnal Geriatri Eur Geriatr Med 2015Dokumen6 halamanJurnal Geriatri Eur Geriatr Med 2015donkeyendutBelum ada peringkat
- Jurnal Geriatri Editorial - Dementia.npsDokumen5 halamanJurnal Geriatri Editorial - Dementia.npsdonkeyendutBelum ada peringkat
- Baru Anthrax - Protocol PDFDokumen13 halamanBaru Anthrax - Protocol PDFdonkeyendutBelum ada peringkat
- Tesis Lampiran Tabel Induk RevisiDokumen1 halamanTesis Lampiran Tabel Induk RevisidonkeyendutBelum ada peringkat
- Jurnal Geriatri Int J Geriatr Psychiatry 2014Dokumen9 halamanJurnal Geriatri Int J Geriatr Psychiatry 2014donkeyendutBelum ada peringkat
- Jurnal 11 CD Manual Anthrax May2012Dokumen4 halamanJurnal 11 CD Manual Anthrax May2012donkeyendutBelum ada peringkat
- Nakamura 2008 Critical CareDokumen2 halamanNakamura 2008 Critical CaredonkeyendutBelum ada peringkat
- Ap 1Dokumen7 halamanAp 1donkeyendutBelum ada peringkat
- Jurnal 1 Impaired Tcell in HIVDokumen9 halamanJurnal 1 Impaired Tcell in HIVdonkeyendutBelum ada peringkat
- Dr. Hendra Ajbr0001-0175Dokumen15 halamanDr. Hendra Ajbr0001-0175donkeyendutBelum ada peringkat
- Tabel Dan Grafik Psiko ACPM 2014Dokumen1 halamanTabel Dan Grafik Psiko ACPM 2014donkeyendutBelum ada peringkat
- Occupational Asthma Occupational Asthma: Sri Handayani LubisDokumen19 halamanOccupational Asthma Occupational Asthma: Sri Handayani LubisdonkeyendutBelum ada peringkat
- Infliximab (Remicade) in The Treatment of Psoriatic ArthritisDokumen12 halamanInfliximab (Remicade) in The Treatment of Psoriatic ArthritisdonkeyendutBelum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Drug Study ErythhropoietinDokumen1 halamanDrug Study ErythhropoietinAkiraMamoBelum ada peringkat
- Anemia of Chronic Disease in The ElderlyDokumen7 halamanAnemia of Chronic Disease in The ElderlyAkbarBelum ada peringkat
- Adams4e Tif Ch31Dokumen19 halamanAdams4e Tif Ch31fbernis1480_11022046Belum ada peringkat
- EpogenDokumen2 halamanEpogenfaizan12233Belum ada peringkat
- Amgen Inc. v. F. Hoffmann-LaRoche LTD Et Al - Document No. 172Dokumen23 halamanAmgen Inc. v. F. Hoffmann-LaRoche LTD Et Al - Document No. 172Justia.comBelum ada peringkat
- Bookchapter-Therapeutic Protein EngineeringDokumen24 halamanBookchapter-Therapeutic Protein EngineeringDurgamadhab SwainBelum ada peringkat
- 2011 Enrollment KitDokumen112 halaman2011 Enrollment KitPhilip BluhBelum ada peringkat
- CNN ExamDokumen167 halamanCNN ExamDiana Negron100% (7)
- Recombinant Human Erythropoietin Stimulates Erythropoiesis Via Division and Differentiation of Progenitor Cells in Bone MarrowDokumen2 halamanRecombinant Human Erythropoietin Stimulates Erythropoiesis Via Division and Differentiation of Progenitor Cells in Bone MarrowGwyn RosalesBelum ada peringkat
- Physiological Adaptation Q&ADokumen17 halamanPhysiological Adaptation Q&AFilipino Nurses CentralBelum ada peringkat
- Literature Review On LeukemiaDokumen8 halamanLiterature Review On Leukemiaafdtukasg100% (2)
- Drug Study Domino, Nikki Y.: Drug Indication Nursing ResponsibilityDokumen7 halamanDrug Study Domino, Nikki Y.: Drug Indication Nursing ResponsibilityKapitan BentongBelum ada peringkat
- Fibrogen, AstraZeneca, Astellas, and The Missing Pyrenees Data.Dokumen15 halamanFibrogen, AstraZeneca, Astellas, and The Missing Pyrenees Data.buyersstrikewpBelum ada peringkat
- Drug StudyDokumen12 halamanDrug StudyJessie Cauilan CainBelum ada peringkat
- Memonic Exam 2Dokumen18 halamanMemonic Exam 2Justine Grace TolentinoBelum ada peringkat
- NCLEXDokumen95 halamanNCLEXKurt Sturgeon67% (3)
- AnemiaDokumen10 halamanAnemiaRamesh VaradharajanBelum ada peringkat
- Effects On Lab Test ResultsDokumen18 halamanEffects On Lab Test Resultsjay5ar5jamorabon5torBelum ada peringkat
- Anemia of Chronic DiseaseDokumen5 halamanAnemia of Chronic DiseaseGufront MustofaBelum ada peringkat
- Pharmabites 9 10 07Dokumen1 halamanPharmabites 9 10 07api-3707097Belum ada peringkat
- NP4 Oncology Acute Biologic Crisis Drill 2Dokumen29 halamanNP4 Oncology Acute Biologic Crisis Drill 2Adriano Odysseus Jon O.Belum ada peringkat
- Medication Guide Epogen (Ee-Po-Jen) (Epoetin Alfa) : What Is The Most Important Information I Should Know About Epogen?Dokumen5 halamanMedication Guide Epogen (Ee-Po-Jen) (Epoetin Alfa) : What Is The Most Important Information I Should Know About Epogen?Josh SingerBelum ada peringkat
- Nature Magazine 7160 - 2007-09-20Dokumen135 halamanNature Magazine 7160 - 2007-09-20Roberto KlesBelum ada peringkat
- Anemia PDFDokumen36 halamanAnemia PDFJABelum ada peringkat
- Darbepoetin AlfaDokumen3 halamanDarbepoetin Alfaapi-3797941Belum ada peringkat
- Chronic Renal FailureDokumen13 halamanChronic Renal FailureAnusha VergheseBelum ada peringkat
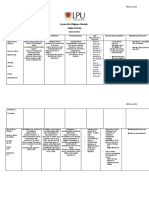
- Lyceum of The Philippines University College of Nursing: MCN Form 014Dokumen3 halamanLyceum of The Philippines University College of Nursing: MCN Form 014twinkleBelum ada peringkat
- JASN 2020 Abstracts PDFDokumen919 halamanJASN 2020 Abstracts PDFrsimranjitBelum ada peringkat
- Case Study For Colon CancerDokumen2 halamanCase Study For Colon Cancerrhimineecat7150% (2)
- Amgen Inc. v. F. Hoffmann-LaRoche LTD Et Al - Document No. 765Dokumen4 halamanAmgen Inc. v. F. Hoffmann-LaRoche LTD Et Al - Document No. 765Justia.comBelum ada peringkat