Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Basic Life Support & First Aid Training ProposalDokumen4 halamanBasic Life Support & First Aid Training ProposalKunle SadareBelum ada peringkat
- Ppa 6 457 PDFDokumen7 halamanPpa 6 457 PDFElizabeth SniderBelum ada peringkat
- Document PDFDokumen5 halamanDocument PDFElizabeth SniderBelum ada peringkat
- Device Therapy in Heart Failure Patients With Chronic Kidney DiseaseDokumen8 halamanDevice Therapy in Heart Failure Patients With Chronic Kidney DiseaseElizabeth SniderBelum ada peringkat
- 1471 2288 11 106 PDFDokumen7 halaman1471 2288 11 106 PDFElizabeth SniderBelum ada peringkat
- Angiotensin-Converting Enzyme Inhibitors and Angiotensin Receptor Blockers in Patients With Congestive Heart Failure and Chronic Kidney DiseaseDokumen10 halamanAngiotensin-Converting Enzyme Inhibitors and Angiotensin Receptor Blockers in Patients With Congestive Heart Failure and Chronic Kidney DiseaseElizabeth SniderBelum ada peringkat
- JC 2010-2756 PDFDokumen12 halamanJC 2010-2756 PDFElizabeth SniderBelum ada peringkat
- Satu Lagi PDFDokumen8 halamanSatu Lagi PDFElizabeth SniderBelum ada peringkat
- Jurnal Metode Analisis Kloramfenikol SalepDokumen10 halamanJurnal Metode Analisis Kloramfenikol SalepCurieJuliaBelum ada peringkat
- Frean1994 PDFDokumen11 halamanFrean1994 PDFElizabeth SniderBelum ada peringkat
- Farmakoterapi PPOK PDFDokumen61 halamanFarmakoterapi PPOK PDFElizabeth SniderBelum ada peringkat
- SFNHS - Extension's School Learning Continuity PlanDokumen5 halamanSFNHS - Extension's School Learning Continuity PlanClaudie MabiniBelum ada peringkat
- Defining Honesty and Integrity: LessonDokumen5 halamanDefining Honesty and Integrity: LessonPetrovichBelum ada peringkat
- Ikigai Worksheet: Passion MissionDokumen1 halamanIkigai Worksheet: Passion Missiontelpastor100% (1)
- Brochure - 3 Months Yoga Cert - 2019-20Dokumen9 halamanBrochure - 3 Months Yoga Cert - 2019-20joga srikanthBelum ada peringkat
- QVASDokumen1 halamanQVASAnjaswati Farida AdyanaBelum ada peringkat
- Chinese Face ReadingDokumen6 halamanChinese Face ReadingGloria GarzaBelum ada peringkat
- Sexual Self Thales ReportDokumen22 halamanSexual Self Thales ReportToni GonzalesBelum ada peringkat
- AvamysDokumen21 halamanAvamysLutfi AyuBelum ada peringkat
- Prevalence of Maxillary Sinus Septa: Systematic Review and Meta-AnalysisDokumen9 halamanPrevalence of Maxillary Sinus Septa: Systematic Review and Meta-AnalysisDennis DinellyBelum ada peringkat
- WHO AIMS 2020 Report On Ghana's Mental Health SystemDokumen64 halamanWHO AIMS 2020 Report On Ghana's Mental Health SystemJustice Kwesi DicksonBelum ada peringkat
- 350 SDS 22feb2023Dokumen8 halaman350 SDS 22feb2023Ying CeBelum ada peringkat
- GOMO Complete Document February 2020 2 242Dokumen1 halamanGOMO Complete Document February 2020 2 242RICROD71Belum ada peringkat
- Sterling Peds Concept MapDokumen6 halamanSterling Peds Concept Mapapi-662884360Belum ada peringkat
- Respiratory Module 4 8Dokumen11 halamanRespiratory Module 4 8David Dwane Art SilorioBelum ada peringkat
- Guidance Calendar of ActivitiesDokumen3 halamanGuidance Calendar of ActivitiesAngelica AlmedaBelum ada peringkat
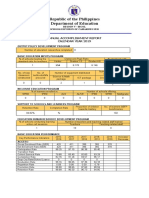
- Republic of The Philippines Department of Education: Annual Accomplishment Report Calendar Year 2019Dokumen4 halamanRepublic of The Philippines Department of Education: Annual Accomplishment Report Calendar Year 2019sheareign dainchylles gamayanBelum ada peringkat
- Back To Balance Heal Your Spine Heal Your LifeDokumen218 halamanBack To Balance Heal Your Spine Heal Your Lifelokita_opdBelum ada peringkat
- Stanley Milgram Case StudyDokumen4 halamanStanley Milgram Case StudyJonathan JohnsonBelum ada peringkat
- Advancement in The Recently Development of Sublingual Tablet For Various Diseases A ReviewDokumen7 halamanAdvancement in The Recently Development of Sublingual Tablet For Various Diseases A ReviewEditor IJTSRDBelum ada peringkat
- 13 - CEORL Fellowship ProgrammeDokumen21 halaman13 - CEORL Fellowship Programmesyed imdadBelum ada peringkat
- LESSON 10. Identifying Different Random Sampling 1Dokumen20 halamanLESSON 10. Identifying Different Random Sampling 1Ian Lorenzo ReyesBelum ada peringkat
- 14 Sustaining Partnerships (DepEd CO-EPS)Dokumen36 halaman14 Sustaining Partnerships (DepEd CO-EPS)Brequillo Bonina MarifeBelum ada peringkat
- J. Mark Elwood, Simon B. Sutcliffe - Cancer Control PDFDokumen484 halamanJ. Mark Elwood, Simon B. Sutcliffe - Cancer Control PDFMartin NovotnyBelum ada peringkat
- Titmus Vision Screener V4Dokumen1 halamanTitmus Vision Screener V4rodrigo rodriguez pachonBelum ada peringkat
- BP Alaska Safety Handbook (BP ASH) PDFDokumen130 halamanBP Alaska Safety Handbook (BP ASH) PDFVan Sot100% (2)
- Fo CBLMDokumen89 halamanFo CBLMJay JayBelum ada peringkat
- Accuracy and Validity of HbA1c POCT Report - August 2020Dokumen86 halamanAccuracy and Validity of HbA1c POCT Report - August 2020Iura FlorinBelum ada peringkat
- University of Central Punjab: Course Title: Performance StrategyDokumen4 halamanUniversity of Central Punjab: Course Title: Performance StrategyAyesha HamidBelum ada peringkat
- Research ProposalDokumen23 halamanResearch ProposalRobelyn AbingBelum ada peringkat