Anda mungkin juga menyukai
- 6th Central Pay Commission Salary CalculatorDokumen15 halaman6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- GMFM 66 Is ScoresheetsDokumen7 halamanGMFM 66 Is ScoresheetsChibulcuteanBelum ada peringkat
- Guide To DBS Stimulation TherapyDokumen61 halamanGuide To DBS Stimulation Therapypratikshah202Belum ada peringkat
- Force Health Protection Nutrition and Exercise ManualDokumen165 halamanForce Health Protection Nutrition and Exercise ManualJared A. Lang100% (1)
- The PresentDokumen138 halamanThe PresentJullyano LinoBelum ada peringkat
- Macrobolic NutritionDokumen65 halamanMacrobolic NutritionBardan RobertBelum ada peringkat
- Niromathe Book en PDFDokumen102 halamanNiromathe Book en PDFChibulcutean0% (1)
- Jekyll HydeDokumen200 halamanJekyll HydeGianini Kroes100% (3)
- Scleroza Multipla-ExercitiiDokumen29 halamanScleroza Multipla-ExercitiigenyyazzBelum ada peringkat
- 475 Kamagon Kamp Roberts KDokumen4 halaman475 Kamagon Kamp Roberts KChibulcuteanBelum ada peringkat
- Brandt Daroff Exercises ML3094Dokumen2 halamanBrandt Daroff Exercises ML3094Chibulcutean50% (2)
- About AmputationDokumen16 halamanAbout AmputationChibulcuteanBelum ada peringkat
- Nia Exercise and Physical Activity PDFDokumen124 halamanNia Exercise and Physical Activity PDFChibulcuteanBelum ada peringkat
- Pliant - MTC Medical Taping QDokumen2 halamanPliant - MTC Medical Taping QChibulcuteanBelum ada peringkat
- 10 2 3 29 EDSS - FormDokumen2 halaman10 2 3 29 EDSS - FormChibulcuteanBelum ada peringkat
- 10 2 3 29 EDSS - FormDokumen2 halaman10 2 3 29 EDSS - FormChibulcuteanBelum ada peringkat
- Core (Medicine Ball)Dokumen33 halamanCore (Medicine Ball)Chibulcutean100% (1)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5782)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (72)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- GRADE 11 PE MODULE 1st QuarterDokumen33 halamanGRADE 11 PE MODULE 1st QuarterDan Paulo BarandaBelum ada peringkat
- Chris Beardsley - Strength Is SpecificDokumen244 halamanChris Beardsley - Strength Is SpecificMarcelo Da Silva100% (5)
- Minor Performance Task Lets Work It OutDokumen4 halamanMinor Performance Task Lets Work It OutArchie GemarinoBelum ada peringkat
- Health Optimizing P.E. Diagnostic TestDokumen28 halamanHealth Optimizing P.E. Diagnostic TestMaria benedicta BenitoBelum ada peringkat
- Research Paper Topics RunningDokumen8 halamanResearch Paper Topics Runningafnhemzabfueaa100% (1)
- 2nd Pathways Ls 2 Answer KeyDokumen31 halaman2nd Pathways Ls 2 Answer KeyHiếu Minh Ngô HoàngBelum ada peringkat
- MedBike SB1Dokumen40 halamanMedBike SB1huntrexBelum ada peringkat
- LmpdbV2 2Dokumen56 halamanLmpdbV2 2lyndon_baker_1100% (1)
- Pe 4 Fun 3 - PDFDokumen47 halamanPe 4 Fun 3 - PDFkhokholBelum ada peringkat
- Fitness Etiquette and Safety ProtocolsDokumen4 halamanFitness Etiquette and Safety ProtocolsJovina Marie NavarroBelum ada peringkat
- HOPE 4 Module 1 Lesson 1Dokumen22 halamanHOPE 4 Module 1 Lesson 1Karelle ArambalaBelum ada peringkat
- Regular Activity DiabetesDokumen10 halamanRegular Activity DiabetesDany RoaBelum ada peringkat
- Unit 1: Lesson 1: Identifying Physical Activities During PandemicDokumen5 halamanUnit 1: Lesson 1: Identifying Physical Activities During PandemicLuna MercedesBelum ada peringkat
- 수특라이트 듣기-1학기 중간Dokumen7 halaman수특라이트 듣기-1학기 중간은총Belum ada peringkat
- CLMD4AHOPESHSDokumen81 halamanCLMD4AHOPESHSkyla mae castilloBelum ada peringkat
- Wyatt Prather - Photo Essay - Physical EducationDokumen17 halamanWyatt Prather - Photo Essay - Physical Educationapi-533348723Belum ada peringkat
- Intermittent Fasting Cheat Sheet PDFDokumen30 halamanIntermittent Fasting Cheat Sheet PDFjong bariquit89% (9)
- Recetas Prácticas de Nutrición para Alto Rendimiento FC BarcelonaDokumen66 halamanRecetas Prácticas de Nutrición para Alto Rendimiento FC BarcelonaVíctor López Me entrena100% (1)
- Applied Principles of Optimal Power DevelopmentDokumen125 halamanApplied Principles of Optimal Power DevelopmentCodi Fitzgerald100% (11)
- Phyed Fitness All in Source by JaysonDokumen173 halamanPhyed Fitness All in Source by JaysonMark De GuzmanBelum ada peringkat
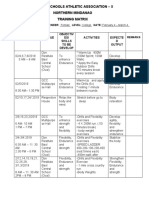
- Private Schools Athletic Association - X Northern Mindanao Training MatrixDokumen2 halamanPrivate Schools Athletic Association - X Northern Mindanao Training MatrixNica Ilano100% (1)
- XII Opt.a Phy. Edu Sample PaperDokumen5 halamanXII Opt.a Phy. Edu Sample Paperococ yamaysaharBelum ada peringkat
- Physical Education: Health - Related FitnessDokumen44 halamanPhysical Education: Health - Related FitnessVlessie Mae Vencer83% (6)
- Back Door Into Hermetics A Guide To Becoming Initiated Into The Mysteries (Mark Rasmus, Jake Senn) (Z-Library)Dokumen161 halamanBack Door Into Hermetics A Guide To Becoming Initiated Into The Mysteries (Mark Rasmus, Jake Senn) (Z-Library)Keenan Griffin100% (1)
- 5 Day Muscle & Strength Building Workout SplitDokumen21 halaman5 Day Muscle & Strength Building Workout Splityoucef mohamedBelum ada peringkat
- Pe 10 - Principles of Physical Fitness - Midterm ExamDokumen5 halamanPe 10 - Principles of Physical Fitness - Midterm ExamJoseph Bernard MarceloBelum ada peringkat
- Basic 1 Manual EnglishDokumen43 halamanBasic 1 Manual EnglishPriteshJadhav100% (1)
- ข้อสอบ A-level ปี 2566 วิชาภาษาอังกฤษ ครบ 80 ข้อ พร้อมเฉลยDokumen30 halamanข้อสอบ A-level ปี 2566 วิชาภาษาอังกฤษ ครบ 80 ข้อ พร้อมเฉลยPatjit KanBelum ada peringkat
- PM5 QuickStartGuide EnglishOnlyDokumen3 halamanPM5 QuickStartGuide EnglishOnlyasperfudBelum ada peringkat
- TG G7Dokumen51 halamanTG G7felekebirhanu7Belum ada peringkat