Anda mungkin juga menyukai
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Disease Spotlight: Diabetes Mellitus: Insulin Insulin Is A Drug That Is Used To ControlDokumen7 halamanDisease Spotlight: Diabetes Mellitus: Insulin Insulin Is A Drug That Is Used To ControlMIR SARTAJBelum ada peringkat
- Motherperpetual Help NovenaDokumen6 halamanMotherperpetual Help NovenaRandyBelum ada peringkat
- ATSP (Asked To See Patient) BookletDokumen24 halamanATSP (Asked To See Patient) BookletCindy WongBelum ada peringkat
- Constitution and By-Laws of The English Club: Article I: Nature and NameDokumen6 halamanConstitution and By-Laws of The English Club: Article I: Nature and NameRandy0% (1)
- Intermittent FastingDokumen14 halamanIntermittent FastingchloevagyokBelum ada peringkat
- Pico PaperDokumen9 halamanPico PaperTraci Braden100% (2)
- E - Cart DrugsDokumen18 halamanE - Cart Drugs'SheenMarkReal'100% (2)
- Organization in ArchitectureDokumen89 halamanOrganization in ArchitectureRandy50% (2)
- Review LiteratureDokumen23 halamanReview LiteratureDrDeepak Pawar50% (4)
- Project Proposal: 1 Parents Teachers Association General Assembly Meeting Cum WINS OrientationDokumen2 halamanProject Proposal: 1 Parents Teachers Association General Assembly Meeting Cum WINS OrientationRandy100% (3)
- NAT Reviewer ScienceDokumen3 halamanNAT Reviewer ScienceRandy100% (1)
- JanubDokumen65 halamanJanubRoel PalmairaBelum ada peringkat
- Clinical Teaching Psychiatric NursingDokumen16 halamanClinical Teaching Psychiatric NursingRandy100% (2)
- RLE Focus - BMC-ER (Revised)Dokumen8 halamanRLE Focus - BMC-ER (Revised)Randy100% (1)
- Core (STEM) - SLM 3-Grade 1112DRRR-1st Quarter-The Effects of DisasterDokumen30 halamanCore (STEM) - SLM 3-Grade 1112DRRR-1st Quarter-The Effects of DisasterRandyBelum ada peringkat
- Unusual Presentation of Pancreatic Insulinoma:a Case ReportDokumen5 halamanUnusual Presentation of Pancreatic Insulinoma:a Case ReportIJAR JOURNALBelum ada peringkat
- Davao Preboard Gen EdDokumen14 halamanDavao Preboard Gen EdRandyBelum ada peringkat
- CertificateDokumen1 halamanCertificateRandyBelum ada peringkat
- Comparison Chart: (Conduction, Convection, Radiation)Dokumen5 halamanComparison Chart: (Conduction, Convection, Radiation)RandyBelum ada peringkat
- A - Step by stepCPRDokumen2 halamanA - Step by stepCPRRandyBelum ada peringkat
- Visual Arts1Dokumen4 halamanVisual Arts1RandyBelum ada peringkat
- Julymar P. Cadacio: Camarines Sur Institute of Fishiries and Marines Science (CASIFMAS) - Ragay BranchDokumen2 halamanJulymar P. Cadacio: Camarines Sur Institute of Fishiries and Marines Science (CASIFMAS) - Ragay BranchRandyBelum ada peringkat
- Figure of SpeechDokumen7 halamanFigure of SpeechRandyBelum ada peringkat
- Apsca Question MapehDokumen10 halamanApsca Question MapehRandyBelum ada peringkat
- Overview of Humanities & ScopeDokumen97 halamanOverview of Humanities & ScopeRandyBelum ada peringkat
- Organization in The Visual ArtsDokumen13 halamanOrganization in The Visual ArtsRandyBelum ada peringkat
- Mapeh SyllabusDokumen7 halamanMapeh SyllabusRandyBelum ada peringkat
- Staging A A Ritual DanceDokumen13 halamanStaging A A Ritual DanceRandyBelum ada peringkat
- Glycemic Targets Standards of Care in Diabetes-2023Dokumen14 halamanGlycemic Targets Standards of Care in Diabetes-2023ÁngelesBelum ada peringkat
- Drug StudyDokumen6 halamanDrug Studydwyane0033Belum ada peringkat
- Signs Alcohol PoisoningDokumen1 halamanSigns Alcohol PoisoningGet TreatmentBelum ada peringkat
- Novorapid Product Monograph PDFDokumen50 halamanNovorapid Product Monograph PDFAtid AmandaBelum ada peringkat
- Iron ToxicityDokumen35 halamanIron ToxicityMohamed El-sayedBelum ada peringkat
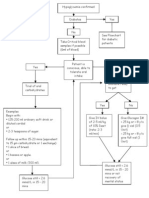
- Hypoglycaemia FlowchartDokumen1 halamanHypoglycaemia FlowchartMohammad SultanBelum ada peringkat
- 5Dokumen41 halaman5myBelum ada peringkat
- The Neonate at 24 To 48 Hours Following Early DischargeDokumen8 halamanThe Neonate at 24 To 48 Hours Following Early Dischargenursereview100% (2)
- Krok I 2013-17 ExplainedDokumen292 halamanKrok I 2013-17 ExplainedU1GoKu0% (1)
- Type 2 Diabetes: Aace Comprehensive Management AlgorithmDokumen10 halamanType 2 Diabetes: Aace Comprehensive Management AlgorithmDiana YaeliBelum ada peringkat
- A Descriptive Study To Assess The Knowledge and Attitude Regarding Self Administration of Insulin Injection Among Diabetes Mellitus Patients in Rural Area at DehradunDokumen5 halamanA Descriptive Study To Assess The Knowledge and Attitude Regarding Self Administration of Insulin Injection Among Diabetes Mellitus Patients in Rural Area at DehradunEditor IJTSRDBelum ada peringkat
- Ins Susp Vial PIL 5Dokumen6 halamanIns Susp Vial PIL 5Kathleen Salvador-RamosBelum ada peringkat
- GlipizideDokumen2 halamanGlipizideFeliciaDorghamBelum ada peringkat
- Lab ValuesDokumen58 halamanLab ValuesAndy GoldstoneBelum ada peringkat
- Drug Study On Agents Used Thyroid and Glucose MetabolismDokumen12 halamanDrug Study On Agents Used Thyroid and Glucose MetabolismBrixean BatacBelum ada peringkat
- Evaluation of Antidiabetic Activity of Aqueous Extract of Mangifera Indica Leaves in Alloxan Induced Diabetic RatsDokumen7 halamanEvaluation of Antidiabetic Activity of Aqueous Extract of Mangifera Indica Leaves in Alloxan Induced Diabetic RatsJethro Floyd QuintoBelum ada peringkat
- Ekstrak MurbeiDokumen23 halamanEkstrak MurbeidarmahadipradiptaBelum ada peringkat
- Synopsis PallaviDokumen31 halamanSynopsis PallaviSanjeet DuhanBelum ada peringkat
- Causes of Hypoglycemia in Infants and ChildrenDokumen18 halamanCauses of Hypoglycemia in Infants and ChildrenhelviBelum ada peringkat
- Protocolo YaleDokumen7 halamanProtocolo Yalegiseladelarosa2006Belum ada peringkat
- Dr. Blyden: Unconscious Person & CPRDokumen72 halamanDr. Blyden: Unconscious Person & CPRBlyden NoahBelum ada peringkat
- IDF T2D CPR 2017 Interactive PDFDokumen43 halamanIDF T2D CPR 2017 Interactive PDFPedro HenriqueBelum ada peringkat