Anda mungkin juga menyukai
- Infection Control Lesson PlanDokumen3 halamanInfection Control Lesson Planapi-305903882100% (3)
- Test Bank ECGs Made Easy 5th Edition Barbara J AehlertDokumen10 halamanTest Bank ECGs Made Easy 5th Edition Barbara J AehlertErnest67% (3)
- Pathophysiology On Liver CirrhosisDokumen38 halamanPathophysiology On Liver CirrhosisYogi AnjasmaraBelum ada peringkat
- Drug Study FluimucilDokumen2 halamanDrug Study FluimucilJemina Rafanan Racadio0% (1)
- SHARONDokumen65 halamanSHARONFaith InstitutionsBelum ada peringkat
- Factors Affecting Antenatal Care Utilization in Yem PDFDokumen7 halamanFactors Affecting Antenatal Care Utilization in Yem PDFNuridha FauziyahBelum ada peringkat
- Procedure Checklist SuctioningDokumen4 halamanProcedure Checklist SuctioningGlaizalyn Fabella Tagoon50% (2)
- Endocrine, Metabolic & Nephrology MCQS: Thyroid Eye DiseaseDokumen78 halamanEndocrine, Metabolic & Nephrology MCQS: Thyroid Eye DiseaseDr.younes95 RekaaneyBelum ada peringkat
- Poster Urine Sediment - GBDokumen1 halamanPoster Urine Sediment - GBROBERTO CESPEDES0% (1)
- Drug StudyDokumen2 halamanDrug Studyluvbel100% (2)
- Neonatal Mortality, Risk Factors and Causes: A Prospective Population-Based Cohort Study in Urban PakistanDokumen10 halamanNeonatal Mortality, Risk Factors and Causes: A Prospective Population-Based Cohort Study in Urban PakistanchinafiBelum ada peringkat
- Neonatal Mortality, Risk Factors and Causes - A Prospective Population-Based Cohort Study in Urban PakistanDokumen7 halamanNeonatal Mortality, Risk Factors and Causes - A Prospective Population-Based Cohort Study in Urban PakistanDavid OlarinloyeBelum ada peringkat
- Neonatal Mortality, Risk Factors and Causes: A Prospective Population-Based Cohort Study in Urban PakistanDokumen18 halamanNeonatal Mortality, Risk Factors and Causes: A Prospective Population-Based Cohort Study in Urban Pakistanermi ellyBelum ada peringkat
- JWH 2006 0295 LowlinkDokumen7 halamanJWH 2006 0295 LowlinkRiskhan VirniaBelum ada peringkat
- Pre Discharge Neonatal Mortality and Morbidity of Extreme Preterm InfantsDokumen4 halamanPre Discharge Neonatal Mortality and Morbidity of Extreme Preterm InfantsDr. Nimesha GamhewageBelum ada peringkat
- A Retrospective Study To Know The Perinatal Mortality Rate and Its Sequence in Nishter Hospital MultanDokumen5 halamanA Retrospective Study To Know The Perinatal Mortality Rate and Its Sequence in Nishter Hospital MultaniajpsBelum ada peringkat
- Jurnal ObgynDokumen10 halamanJurnal ObgynUgi RahulBelum ada peringkat
- Cause-Specific Child Mortality in A Mountainous Community in Pakistan by Verbal AutopsyDokumen8 halamanCause-Specific Child Mortality in A Mountainous Community in Pakistan by Verbal AutopsyDr. Muhammad Bilal SiddiquiBelum ada peringkat
- Hernandez, Et Al.Dokumen11 halamanHernandez, Et Al.Yet Barreda BasbasBelum ada peringkat
- Analytical Study of Intrauterine Fetal Death Cases and Associated Maternal ConditionsDokumen5 halamanAnalytical Study of Intrauterine Fetal Death Cases and Associated Maternal ConditionsNurvita WidyastutiBelum ada peringkat
- A Prospective Cohort Study of Pregnancy Risk Factors and Birth Outcomes in Aboriginal WomenDokumen5 halamanA Prospective Cohort Study of Pregnancy Risk Factors and Birth Outcomes in Aboriginal WomenFirman DariyansyahBelum ada peringkat
- An Intervention Involving Traditional Birth Attendants and Perinatal and Maternal Mortality in PakistanDokumen9 halamanAn Intervention Involving Traditional Birth Attendants and Perinatal and Maternal Mortality in PakistanAndaru Kusuma PrajaBelum ada peringkat
- Neonatal and Obstetric Risk Assessment (NORA) Pregnancy Cohort Study in SingaporeDokumen7 halamanNeonatal and Obstetric Risk Assessment (NORA) Pregnancy Cohort Study in SingaporePremier PublishersBelum ada peringkat
- Factors Associated With Home Maternal Deliveries in Rural AreasDokumen24 halamanFactors Associated With Home Maternal Deliveries in Rural AreasJASH MATHEW100% (1)
- Morbidly Adherent Placenta Treatments and OutcomesDokumen15 halamanMorbidly Adherent Placenta Treatments and OutcomesDara Mayang SariBelum ada peringkat
- Pmed 1002547Dokumen21 halamanPmed 1002547Louinel JosephBelum ada peringkat
- 247-Article Text-1425-1-10-20200122Dokumen11 halaman247-Article Text-1425-1-10-20200122Gisela M SilvaBelum ada peringkat
- Early Prediction of Preterm Birth For Singleton, Twin, and Triplet PregnanciesDokumen6 halamanEarly Prediction of Preterm Birth For Singleton, Twin, and Triplet PregnanciesNi Wayan Ana PsBelum ada peringkat
- 9 JurnalDokumen83 halaman9 JurnalWanda AndiniBelum ada peringkat
- Jembeng CDDDDJDJDJDokumen7 halamanJembeng CDDDDJDJDJAlzamri FhilzaBelum ada peringkat
- Effectiveness of Antenatal Care Package On Knowledge of Pregnancy Induced HypertensionDokumen3 halamanEffectiveness of Antenatal Care Package On Knowledge of Pregnancy Induced Hypertensionazida90Belum ada peringkat
- 2.april 2020 Estimation of Risk Factors For MultiparousDokumen4 halaman2.april 2020 Estimation of Risk Factors For MultiparousTushar BahetiBelum ada peringkat
- Parturition Events and Risk of Urinary Incontinence in Later LifeDokumen16 halamanParturition Events and Risk of Urinary Incontinence in Later LifeMutia LailaniBelum ada peringkat
- Ectopic Pregnancy and Its Effect On Future Fertility: Original StudiesDokumen0 halamanEctopic Pregnancy and Its Effect On Future Fertility: Original StudiesnajmulBelum ada peringkat
- Severe Birth Asphyxia: Risk Factors As Seen in A Tertiary Institution in The Niger Delta Area of NigeriaDokumen9 halamanSevere Birth Asphyxia: Risk Factors As Seen in A Tertiary Institution in The Niger Delta Area of NigeriaSteven JonesBelum ada peringkat
- Antenatal CareDokumen10 halamanAntenatal CareBachtiar M TaUfikBelum ada peringkat
- Jurnal HivDokumen9 halamanJurnal Hivsheva25Belum ada peringkat
- Transcultural NursingDokumen1 halamanTranscultural NursingTharangaBelum ada peringkat
- The Influence of Distance and Quality of Care On Place of Delivery in Rural GhanaDokumen8 halamanThe Influence of Distance and Quality of Care On Place of Delivery in Rural GhanaJames Czar FontanillaBelum ada peringkat
- Women's Health-What's New Worldwide: International Guidelines, Patents and TrialsDokumen3 halamanWomen's Health-What's New Worldwide: International Guidelines, Patents and TrialsGladstone AsadBelum ada peringkat
- Frequency of Uterine Contractions and The Risk of Spontaneous Preterm DeliveryDokumen7 halamanFrequency of Uterine Contractions and The Risk of Spontaneous Preterm DeliveryiullBelum ada peringkat
- Hie GoodDokumen8 halamanHie GoodIkhaAnggieeBelum ada peringkat
- A Descriptive Study Was Undertaken To Gain Insight Into The Knowledge Base of Expectant Mother's Attending Antenatal OPD at A Selected Hospital in The State of Uttar PradeshDokumen5 halamanA Descriptive Study Was Undertaken To Gain Insight Into The Knowledge Base of Expectant Mother's Attending Antenatal OPD at A Selected Hospital in The State of Uttar PradeshInternational Journal of Innovative Science and Research TechnologyBelum ada peringkat
- Peripartum Hysterectomy: A Life Saving Procedure: Original ArticleDokumen4 halamanPeripartum Hysterectomy: A Life Saving Procedure: Original ArticleEdwin MasholaBelum ada peringkat
- Analysis of Mortality in PICU of A Tertiary Care Teaching Hospital, Telangana - An IntrospectionDokumen29 halamanAnalysis of Mortality in PICU of A Tertiary Care Teaching Hospital, Telangana - An IntrospectionRusmila UlfahBelum ada peringkat
- Aborto MedicoDokumen6 halamanAborto MedicoJen OjedaBelum ada peringkat
- Contemporary Cesarean Delivery Practice in The United StatesDokumen17 halamanContemporary Cesarean Delivery Practice in The United StatesdedypurnamaBelum ada peringkat
- Singleton Term Breech Deliveries in Nulliparous and Multiparous Women: A 5-Year Experience at The University of Miami/Jackson Memorial HospitalDokumen6 halamanSingleton Term Breech Deliveries in Nulliparous and Multiparous Women: A 5-Year Experience at The University of Miami/Jackson Memorial HospitalSarah SilaenBelum ada peringkat
- Assessment of Fresh Vs Macerated As Acurate Markers of Time Since IUFD in Low-Income CountriesDokumen5 halamanAssessment of Fresh Vs Macerated As Acurate Markers of Time Since IUFD in Low-Income CountriesDenys PutraBelum ada peringkat
- CIH2005 2 AKalaichandran MaternalMortalityDokumen11 halamanCIH2005 2 AKalaichandran MaternalMortalityMustaf MohamedBelum ada peringkat
- The Role of Son Preference in Reproductive Behaviour in PakistanDokumen10 halamanThe Role of Son Preference in Reproductive Behaviour in Pakistanbilal rajputBelum ada peringkat
- Comparative Study of Nifedipine and Isoxpurine As Tocolytics For Preterm LaborDokumen4 halamanComparative Study of Nifedipine and Isoxpurine As Tocolytics For Preterm LaborMeitika Wahyu Wedha WatiBelum ada peringkat
- McDonald Et Al-2015-BJOG - An International Journal of Obstetrics & GynaecologyDokumen8 halamanMcDonald Et Al-2015-BJOG - An International Journal of Obstetrics & GynaecologyKevin LoboBelum ada peringkat
- 33873-Article Text-121761-1-10-20170831Dokumen6 halaman33873-Article Text-121761-1-10-20170831AnggaBelum ada peringkat
- Pregnancy at Very Advanced Maternal Age: A UK Population-Based Cohort StudyDokumen10 halamanPregnancy at Very Advanced Maternal Age: A UK Population-Based Cohort StudyDM A27 RSU Haji SUBBelum ada peringkat
- Ectopic Pregnancy Incidence in The Republic of KoreaDokumen5 halamanEctopic Pregnancy Incidence in The Republic of KoreaJustin IqbalBelum ada peringkat
- Art:10.1186/1471 2393 14 337 PDFDokumen10 halamanArt:10.1186/1471 2393 14 337 PDF<_>Belum ada peringkat
- Original ArticleDokumen6 halamanOriginal Articlerajforever17Belum ada peringkat
- ViabilityDokumen10 halamanViabilityapi-282195779Belum ada peringkat
- Salinan Terjemahan 808-1523-1-SMDokumen17 halamanSalinan Terjemahan 808-1523-1-SMfatmah rifathBelum ada peringkat
- Research: Birth Preparedness and Complication Readiness Among WomenDokumen5 halamanResearch: Birth Preparedness and Complication Readiness Among WomenJyothi RameshBelum ada peringkat
- ProQuestDocuments 2018 08 18 PDFDokumen3 halamanProQuestDocuments 2018 08 18 PDFUtama puteraBelum ada peringkat
- AsdasfasfvDokumen7 halamanAsdasfasfvPulseWangminBelum ada peringkat
- P ('t':'3', 'I':'3053721863') D '' Var B Location Settimeout (Function ( If (Typeof Window - Iframe 'Undefined') ( B.href B.href ) ), 15000)Dokumen3 halamanP ('t':'3', 'I':'3053721863') D '' Var B Location Settimeout (Function ( If (Typeof Window - Iframe 'Undefined') ( B.href B.href ) ), 15000)Ni Wayan Ana PsBelum ada peringkat
- Accepted ManuscriptDokumen27 halamanAccepted ManuscriptsilvanaBelum ada peringkat
- Antenatal Betamethasone For Women at RiskDokumen10 halamanAntenatal Betamethasone For Women at RiskThapakorn JalearnyingBelum ada peringkat
- Knowledge, Attitudes, and Perceptions of Preeclampsia Among First-Generation Nigerian Women in the United StatesDari EverandKnowledge, Attitudes, and Perceptions of Preeclampsia Among First-Generation Nigerian Women in the United StatesBelum ada peringkat
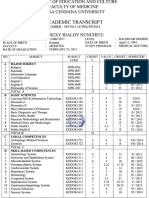
- Transkrip InggrisDokumen2 halamanTranskrip InggrisRexy NunuhituBelum ada peringkat
- BCJLSF Yes No: Title First Name Last Name Pax Type Lion Passport # Eticket #Dokumen1 halamanBCJLSF Yes No: Title First Name Last Name Pax Type Lion Passport # Eticket #Rexy NunuhituBelum ada peringkat
- Anti Retro ViralDokumen6 halamanAnti Retro ViralRexy NunuhituBelum ada peringkat
- Bruno Mars - Just The Way You Are LyricsDokumen9 halamanBruno Mars - Just The Way You Are LyricsRexy NunuhituBelum ada peringkat
- BFG (M249 SAW) in City Streets LevelDokumen5 halamanBFG (M249 SAW) in City Streets LevelRexy NunuhituBelum ada peringkat
- Def JamDokumen14 halamanDef JamRexy NunuhituBelum ada peringkat
- 14 IngDokumen6 halaman14 IngRexy NunuhituBelum ada peringkat
- Kuliah DR - EkaDokumen26 halamanKuliah DR - EkaRexy NunuhituBelum ada peringkat
- CA Treatment Phyllodes Web AlgorithmDokumen4 halamanCA Treatment Phyllodes Web AlgorithmNurul Ramadhani IslamiBelum ada peringkat
- Magnesium Sulfat: Maisuri T. ChalidDokumen23 halamanMagnesium Sulfat: Maisuri T. ChalidDevy Oktavia AnisaBelum ada peringkat
- ScoliosisDokumen99 halamanScoliosismarjan dronjakBelum ada peringkat
- Arthrogryposis Multiplex Congenita-Dr S P DasDokumen7 halamanArthrogryposis Multiplex Congenita-Dr S P DasSheel GuptaBelum ada peringkat
- Aerobic and Anaerobic ExercisesDokumen3 halamanAerobic and Anaerobic ExercisesBonak na BataBelum ada peringkat
- Growth Faltering, Puberty and Growth ChartsDokumen4 halamanGrowth Faltering, Puberty and Growth ChartsCaine ReganBelum ada peringkat
- 1000 Ques & Ans File 2Dokumen54 halaman1000 Ques & Ans File 2bibin joyBelum ada peringkat
- Assessment of Knowledge, Attitude and Awareness Regarding Cone Beam Computed Tomography Among Dental Graduates in Pune City, IndiaDokumen5 halamanAssessment of Knowledge, Attitude and Awareness Regarding Cone Beam Computed Tomography Among Dental Graduates in Pune City, IndiaSakina JigarBelum ada peringkat
- Antibiotic Prophylaxis in Dentistry: A Review and Practice RecommendationsDokumen9 halamanAntibiotic Prophylaxis in Dentistry: A Review and Practice RecommendationsDina AnisawatiBelum ada peringkat
- The Benefits of Immunotherapy CombinationsDokumen1 halamanThe Benefits of Immunotherapy CombinationsMicheleFontanaBelum ada peringkat
- Greene & Manfredini 2023 - Overtreatment Successes - 230709 - 135204Dokumen11 halamanGreene & Manfredini 2023 - Overtreatment Successes - 230709 - 135204Abigail HernándezBelum ada peringkat
- Relapsing Polychondritis Case Presentaion Feb 2009 DR - BugnahDokumen21 halamanRelapsing Polychondritis Case Presentaion Feb 2009 DR - BugnahDr.Sherif Bugnah100% (4)
- Test Bank For Pathophysiology 6th Edition Jacquelyn L BanasikDokumen5 halamanTest Bank For Pathophysiology 6th Edition Jacquelyn L BanasikJesus Carter97% (30)
- Epidemiology of Sarcopenia Prevalence, Risk FactoDokumen9 halamanEpidemiology of Sarcopenia Prevalence, Risk FactoW Antonio Rivera MartínezBelum ada peringkat
- Hubungan Pengelolaan Air Minum Dan Makanan Rumah Tangga Dengan Kejadian DiareDokumen6 halamanHubungan Pengelolaan Air Minum Dan Makanan Rumah Tangga Dengan Kejadian DiareAmbar WatiBelum ada peringkat
- Normal Spontaneous DeliveryDokumen4 halamanNormal Spontaneous Deliveryvivian magnoBelum ada peringkat
- Pathological Condition in Buffalo GenitalsDokumen3 halamanPathological Condition in Buffalo GenitalsgnpobsBelum ada peringkat
- Abegail Joy B. Manlunas BS Psychology: Endocrine System Organ Hormone Function Disorder If Too High Disorder If Too LowDokumen4 halamanAbegail Joy B. Manlunas BS Psychology: Endocrine System Organ Hormone Function Disorder If Too High Disorder If Too LowabegailmanlunasBelum ada peringkat
- Therapy With Physical Exercise in The Treatment of Chikugunya in The Chronic PhaseDokumen5 halamanTherapy With Physical Exercise in The Treatment of Chikugunya in The Chronic PhaseNailton Albuquerque FilhoBelum ada peringkat
- Examination of The SkinDokumen24 halamanExamination of The SkinRay Christoffer GomezBelum ada peringkat
- A Review of The New GLP-1 Receptor Agonist/basal Insulin Fixed-Ratio Combination ProductsDokumen11 halamanA Review of The New GLP-1 Receptor Agonist/basal Insulin Fixed-Ratio Combination Productsarief hakikiBelum ada peringkat
- Dams Video Based TestDokumen30 halamanDams Video Based TestPandey AyushBelum ada peringkat