Anda mungkin juga menyukai
- Networking A Beginner's GuideDokumen36 halamanNetworking A Beginner's Guidez4rm4rBelum ada peringkat
- Electrolyte DisordersDokumen10 halamanElectrolyte DisordersSlavicaBelum ada peringkat
- AnaesthesiaDokumen121 halamanAnaesthesiaSandeep Bhangale100% (1)
- Dell Inspiron 17 5755 Compal LA-C142P r1.0 AMDDokumen56 halamanDell Inspiron 17 5755 Compal LA-C142P r1.0 AMDWarren Donaldson100% (1)
- (Pathophysiology, Types & MGT) : ShockDokumen37 halaman(Pathophysiology, Types & MGT) : ShockApriliani Nur Puspita SariBelum ada peringkat
- Vasodilators by Hiren PatelDokumen28 halamanVasodilators by Hiren PatelHiren_Patel_2427Belum ada peringkat
- Josephine Morrow: Guided Reflection QuestionsDokumen3 halamanJosephine Morrow: Guided Reflection QuestionsElliana Ramirez100% (1)
- Acid-Base and Electrolyte Handbook for Veterinary TechniciansDari EverandAcid-Base and Electrolyte Handbook for Veterinary TechniciansAngela Randels-ThorpBelum ada peringkat
- Hypovolemic ShockDokumen8 halamanHypovolemic ShockLyka Flores100% (1)
- Perfusion for Congenital Heart Surgery: Notes on Cardiopulmonary Bypass for a Complex Patient PopulationDari EverandPerfusion for Congenital Heart Surgery: Notes on Cardiopulmonary Bypass for a Complex Patient PopulationPenilaian: 5 dari 5 bintang5/5 (2)
- Institutional Biosafety Committee: Role of TheDokumen14 halamanInstitutional Biosafety Committee: Role of TheSyeda Wardah NoorBelum ada peringkat
- Chapter 66 - ShockDokumen9 halamanChapter 66 - ShockCrysta Venice Tapoc100% (1)
- Fluids Concept MappingDokumen1 halamanFluids Concept Mappingmariagarcia415100% (1)
- 04 ShockDokumen142 halaman04 ShockDefa3 madniBelum ada peringkat
- Interpretation of Arterial Blood Gases (Abgs) I David A. Kaufman, MD DDokumen17 halamanInterpretation of Arterial Blood Gases (Abgs) I David A. Kaufman, MD DingridpuspitaBelum ada peringkat
- Med Surg QuizDokumen91 halamanMed Surg QuizCharles Gerard B. Beluan0% (1)
- Shock 2022 SeminarDokumen17 halamanShock 2022 Seminarrosie100% (2)
- Evaluation of Outpatient Department in A Public Super Speciality Hospital in IndiaDokumen4 halamanEvaluation of Outpatient Department in A Public Super Speciality Hospital in IndiaMadhusudan MBelum ada peringkat
- Pre-Eclampsia and EclampsiaDokumen21 halamanPre-Eclampsia and EclampsiaTamratKelelegn100% (1)
- NMC CBT SAMPLE Q&A PART 3 KEY NURSING CONCEPTSDokumen14 halamanNMC CBT SAMPLE Q&A PART 3 KEY NURSING CONCEPTSJoane FranciscoBelum ada peringkat
- Dialysis Treatment Options and IndicationsDokumen66 halamanDialysis Treatment Options and Indicationsjoms_pasanoBelum ada peringkat
- ShockDokumen49 halamanShockpaulyn ramos100% (1)
- Shock Types 141009102815 Conversion Gate01Dokumen41 halamanShock Types 141009102815 Conversion Gate01Samjaisheel SamsonBelum ada peringkat
- Fluid Therapy FinalDokumen3 halamanFluid Therapy Finallaureeate100% (1)
- Conivaptan MedicalDokumen38 halamanConivaptan MedicalSanjay NavaleBelum ada peringkat
- First aid and treatment for hypovolemia from blood lossDokumen5 halamanFirst aid and treatment for hypovolemia from blood lossIan Rama100% (1)
- Hemorrhagic ShockDokumen5 halamanHemorrhagic ShockGhina RahmadiantiBelum ada peringkat
- 82 Siadh PDFDokumen10 halaman82 Siadh PDFSalsabilla SaharaBelum ada peringkat
- Bhatia ElectrolytesDokumen5 halamanBhatia Electrolytesnaga tanoojBelum ada peringkat
- MTE Diagnosis and Manag ShockDokumen52 halamanMTE Diagnosis and Manag ShockGarbha JmrsBelum ada peringkat
- Shock in The Pediatric Patient: or Oxygen Don't Go Where The Blood Won't Flow!Dokumen63 halamanShock in The Pediatric Patient: or Oxygen Don't Go Where The Blood Won't Flow!Nishanth BabuBelum ada peringkat
- Common Electrolyte Disturbance Their Management and Anesthesia ConsiderationDokumen65 halamanCommon Electrolyte Disturbance Their Management and Anesthesia ConsiderationagatakassaBelum ada peringkat
- 4 - Hypothalmus - Post PituitaryDokumen21 halaman4 - Hypothalmus - Post PituitaryAbboodBelum ada peringkat
- Overview of Acid-Base and Electrolyte Disorders: The Right Clinical Information, Right Where It's NeededDokumen14 halamanOverview of Acid-Base and Electrolyte Disorders: The Right Clinical Information, Right Where It's NeededNelvinBaezMelendrezBelum ada peringkat
- Manajemen ShockDokumen47 halamanManajemen ShockPutry RizqiaBelum ada peringkat
- Shock: By: Dr. Samer Sabri M.B.CH.B F.I.C.M.SDokumen34 halamanShock: By: Dr. Samer Sabri M.B.CH.B F.I.C.M.Ssamer falconBelum ada peringkat
- Hemorrhagic ShockDokumen2 halamanHemorrhagic ShockPharhana PuterieBelum ada peringkat
- Electrolyte Disorders: Jai Radhakrishnan, MDDokumen46 halamanElectrolyte Disorders: Jai Radhakrishnan, MDAnobee EbenizaBelum ada peringkat
- Fluid and Electrolyte DisordersDokumen49 halamanFluid and Electrolyte DisordersKholoud KholoudBelum ada peringkat
- SHOCKDokumen28 halamanSHOCKMohammad Azzlan Abd RahmanBelum ada peringkat
- SHOCK GUIDEDDokumen70 halamanSHOCK GUIDEDrajevikramBelum ada peringkat
- Shock Five Point ZeroDokumen78 halamanShock Five Point ZeroprashsubbuBelum ada peringkat
- DR - Nursamsu, SpPD-KGH-Penggunaan Cairan Koloid Pada Kondisi Syok PDFDokumen38 halamanDR - Nursamsu, SpPD-KGH-Penggunaan Cairan Koloid Pada Kondisi Syok PDFNONABelum ada peringkat
- Identifying Types of Shock in Dogs & Cats - Site - NameDokumen8 halamanIdentifying Types of Shock in Dogs & Cats - Site - Namelara yaseenBelum ada peringkat
- Pathophysiology of Shock: Microcirculation, Cellular Responses, and Organ DysfunctionDokumen22 halamanPathophysiology of Shock: Microcirculation, Cellular Responses, and Organ DysfunctionMohamad Rizki DwikaneBelum ada peringkat
- Shock: (Pathophysiology, Types & MGT)Dokumen37 halamanShock: (Pathophysiology, Types & MGT)yusufBelum ada peringkat
- Hyponatremia in Cirrhosis: An Update: Joseph J. Alukal, MD, Savio John, MD and Paul J. Thuluvath, MD, FRCPDokumen11 halamanHyponatremia in Cirrhosis: An Update: Joseph J. Alukal, MD, Savio John, MD and Paul J. Thuluvath, MD, FRCPMuzaffar MehdiBelum ada peringkat
- Ijem 18 760Dokumen12 halamanIjem 18 760HafizahLatifBelum ada peringkat
- MINI ReviewDokumen10 halamanMINI ReviewShamila KaruthuBelum ada peringkat
- Fluids and Electrolytes-SeminarDokumen119 halamanFluids and Electrolytes-Seminarنديم الباهليBelum ada peringkat
- Management of Paediatric Shock - Fluids and InotropesDokumen78 halamanManagement of Paediatric Shock - Fluids and InotropesRahmanu ReztaputraBelum ada peringkat
- 1 - Chap13-Fluid and Electrolyte - Balance and Disturbance 2017Dokumen97 halaman1 - Chap13-Fluid and Electrolyte - Balance and Disturbance 2017ahmadBelum ada peringkat
- Homeostasis: The Kidneys' Role in Fluid and Electrolyte BalanceDokumen56 halamanHomeostasis: The Kidneys' Role in Fluid and Electrolyte BalanceJennBelum ada peringkat
- Circulatory Failure: Shock: Dr. Qusai Al-JarrahDokumen47 halamanCirculatory Failure: Shock: Dr. Qusai Al-JarrahQusai Al JarrahBelum ada peringkat
- Year in Review 2012: Critical Care - CardiologyDokumen6 halamanYear in Review 2012: Critical Care - CardiologyUdrea NicolaeBelum ada peringkat
- Shock Is The Clinical Syndrome That Results FromDokumen43 halamanShock Is The Clinical Syndrome That Results Fromnathan asfahaBelum ada peringkat
- Dr. Sunatrio - Management Hypovolemic ShockDokumen59 halamanDr. Sunatrio - Management Hypovolemic ShockArga Putra SaboeBelum ada peringkat
- ShockDokumen4 halamanShockKrizza Edejer TrillanaBelum ada peringkat
- Edema: Dr. Bernardo Dámaso MataDokumen55 halamanEdema: Dr. Bernardo Dámaso MataDeivis Dan ErickBelum ada peringkat
- History and Current Perspectives of HemodialysisDokumen66 halamanHistory and Current Perspectives of HemodialysisBasharat KarimBelum ada peringkat
- HemodialysisDokumen66 halamanHemodialysisLiliana Wood100% (1)
- Fluid Therapy - 2021Dokumen10 halamanFluid Therapy - 2021Madiha MadiBelum ada peringkat
- Jurnal Penatalaksanaan EdemaDokumen7 halamanJurnal Penatalaksanaan EdemaMariska Nada Debora100% (1)
- Fluid and Electrolyte - SauravDokumen61 halamanFluid and Electrolyte - SauravUsmle GuyBelum ada peringkat
- Electrolyte and Acid Base BalanceDokumen26 halamanElectrolyte and Acid Base BalanceMysheb SSBelum ada peringkat
- Hypovolemic ShockDokumen27 halamanHypovolemic Shock'govamaniacs' Insave IVBelum ada peringkat
- FiiiiiiixDokumen22 halamanFiiiiiiixYeni dwi anggra sudarmajiBelum ada peringkat
- Electrolyte Abnormalities in The Hospitalized PatientDokumen70 halamanElectrolyte Abnormalities in The Hospitalized PatientClaudiaBelum ada peringkat
- Dell Inspirion 15 5551 Compal LA-B912P r1.0Dokumen42 halamanDell Inspirion 15 5551 Compal LA-B912P r1.0Warren DonaldsonBelum ada peringkat
- Social Media and Its Origins SMDokumen8 halamanSocial Media and Its Origins SMWarren DonaldsonBelum ada peringkat
- 6457.PCB LayoutDokumen6 halaman6457.PCB LayoutWarren DonaldsonBelum ada peringkat
- LG TFT-LCD Color Monitor FLATRON W1934S PDFDokumen49 halamanLG TFT-LCD Color Monitor FLATRON W1934S PDFCriss AlbuBelum ada peringkat
- Pmos and CmosDokumen3 halamanPmos and CmosViet NguyenBelum ada peringkat
- #920-0120 Interface BoardDokumen18 halaman#920-0120 Interface BoardKeyBelum ada peringkat
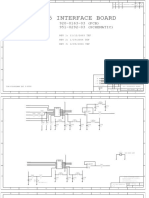
- Q45 Interface Board Schematic and PCB DrawingDokumen26 halamanQ45 Interface Board Schematic and PCB DrawingWarren DonaldsonBelum ada peringkat
- N82 - RADIO (N82 HSDPA RADIO DEV3) Rev 03, 08.16.2007Dokumen17 halamanN82 - RADIO (N82 HSDPA RADIO DEV3) Rev 03, 08.16.2007aplus guideBelum ada peringkat
- Fly Vision Iq300 SchematicsDokumen9 halamanFly Vision Iq300 SchematicsWarren DonaldsonBelum ada peringkat
- Jesus Second ComingDokumen29 halamanJesus Second ComingWarren DonaldsonBelum ada peringkat
- Next7P12-GP Tablet SpecificationDokumen4 halamanNext7P12-GP Tablet SpecificationWarren DonaldsonBelum ada peringkat
- Samsung Gt-p3100 r0.6 SchematicsDokumen11 halamanSamsung Gt-p3100 r0.6 SchematicsWarren Donaldson100% (1)
- Diabetic Conference 2 (1) RenalDokumen20 halamanDiabetic Conference 2 (1) RenalWarren DonaldsonBelum ada peringkat
- Business PlanDokumen21 halamanBusiness PlanWarren DonaldsonBelum ada peringkat
- College Wise P3Dokumen13 halamanCollege Wise P3abdullah khalidBelum ada peringkat
- 43 Adaptive Support Ventilation As VDokumen5 halaman43 Adaptive Support Ventilation As Vnanang criztaBelum ada peringkat
- ILC 2022 Abstract Book 08.06.2022Dokumen1.104 halamanILC 2022 Abstract Book 08.06.2022Helena AlvesBelum ada peringkat
- Anaesthetic Considerations for Day Care SurgeryDokumen8 halamanAnaesthetic Considerations for Day Care SurgerySirisha Ckv100% (1)
- Manajemen Pre-Operatif Pasien Dengan DMDokumen12 halamanManajemen Pre-Operatif Pasien Dengan DMyanayas28Belum ada peringkat
- NCM 104 - Bag TechniqueDokumen2 halamanNCM 104 - Bag TechniqueIrish Margareth AdarloBelum ada peringkat
- The Benefits of TelemedicineDokumen2 halamanThe Benefits of TelemedicineNirat Patel100% (1)
- Aesthetic Medicine Training CourseDokumen8 halamanAesthetic Medicine Training Coursedrdahabra3Belum ada peringkat
- Evmlu Uganda.2020Dokumen124 halamanEvmlu Uganda.2020ALINOMUGASHA EMMANUELBelum ada peringkat
- Heart Failure: Definition, Classification, Epidemiology & PathophysiologyDokumen10 halamanHeart Failure: Definition, Classification, Epidemiology & PathophysiologyAlbert ShantoBelum ada peringkat
- Contoh Nursing Care PlanDokumen1 halamanContoh Nursing Care PlanResmi LindaBelum ada peringkat
- Manual Reprocessing Final Version 2.0Dokumen29 halamanManual Reprocessing Final Version 2.0Enaj AzilgBelum ada peringkat
- Mouth Throat Nose and Sinuses Assessment FindingsDokumen5 halamanMouth Throat Nose and Sinuses Assessment FindingsChris SmithBelum ada peringkat
- Implementing Evidence-Based Decisions in Clinical Practice: Elliot AbtDokumen7 halamanImplementing Evidence-Based Decisions in Clinical Practice: Elliot AbtSri Hari100% (1)
- Sinusitis LectureDokumen66 halamanSinusitis LectureDada Doni100% (2)
- Cons Study Summary QuiestionsDokumen124 halamanCons Study Summary QuiestionsCons Miyu HimeBelum ada peringkat
- LP2 MAJOR EXAM 4 Files Merged 2 Files MergedDokumen285 halamanLP2 MAJOR EXAM 4 Files Merged 2 Files MergedBianca ArceBelum ada peringkat
- Tinnitus Today December 1998 Vol 23, No 4Dokumen29 halamanTinnitus Today December 1998 Vol 23, No 4American Tinnitus AssociationBelum ada peringkat
- PFR Standardsمعايير حقوق المرضى سباهي مترجمة pdfDokumen15 halamanPFR Standardsمعايير حقوق المرضى سباهي مترجمة pdfMohammed YounisBelum ada peringkat
- DSHS Letter To Bowie County Judge GA-32 50 Percent Occupancy For BusinessesDokumen2 halamanDSHS Letter To Bowie County Judge GA-32 50 Percent Occupancy For BusinessesField WalshBelum ada peringkat
- NUTR4320FINAL11Dokumen10 halamanNUTR4320FINAL11rijzBelum ada peringkat
- Hydroxyzine GuidelinesDokumen13 halamanHydroxyzine GuidelinesMahim JainBelum ada peringkat
- Supreme Court Directs UP Govt to Stop Unqualified Medical PractitionersDokumen12 halamanSupreme Court Directs UP Govt to Stop Unqualified Medical PractitionersShakshi MehtaBelum ada peringkat
- EphedraDokumen9 halamanEphedraapi-367367047Belum ada peringkat