Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Pathology MCQDokumen42 halamanPathology MCQJim Jose Antony100% (17)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Common Diseases of NewbornDokumen162 halamanCommon Diseases of NewbornMichelle ThereseBelum ada peringkat
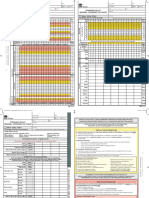
- SAGO AdultObsDokumen2 halamanSAGO AdultObsTim BrownBelum ada peringkat
- Definition, Classification, Etiology, and Pathophysiology of Shock in Adults - UpToDateDokumen20 halamanDefinition, Classification, Etiology, and Pathophysiology of Shock in Adults - UpToDateEstructuración Técnica 2019Belum ada peringkat
- Early Identification and Treatment of SepsisDokumen4 halamanEarly Identification and Treatment of SepsisAnonymous QPakSNBelum ada peringkat
- Bactec BD BacT Alert VersaDokumen10 halamanBactec BD BacT Alert VersaAlejandro Fonseca MillanBelum ada peringkat
- Management of Odontogenic Infections and SepsisDokumen8 halamanManagement of Odontogenic Infections and Sepsismartha carolina vargas bernalBelum ada peringkat
- Nihms520302 PDFDokumen15 halamanNihms520302 PDFArifudin Cipto HusodoBelum ada peringkat
- SepsisDokumen63 halamanSepsisIssela MilagrosBelum ada peringkat
- Types of ShocksDokumen33 halamanTypes of Shocksmark OrpillaBelum ada peringkat
- Gambaran Klinis Dan Tatalaksana SepsisDokumen35 halamanGambaran Klinis Dan Tatalaksana SepsisyunielsyaBelum ada peringkat
- OCR BlueprintsSeries PediatricInfectiousDiseases2004ShahDokumen237 halamanOCR BlueprintsSeries PediatricInfectiousDiseases2004ShahAnthonyJohanBelum ada peringkat
- MCQ1FULLDokumen176 halamanMCQ1FULLtheintrov100% (11)
- Surprised Samples With Coaching Samples (1) 2Dokumen55 halamanSurprised Samples With Coaching Samples (1) 2EmmanuellaBelum ada peringkat
- 10 Respuestas para Manejo de LíquidosDokumen11 halaman10 Respuestas para Manejo de Líquidosfrida casdelBelum ada peringkat
- Common Newborn Problems (2) C1Dokumen39 halamanCommon Newborn Problems (2) C1ZmBelum ada peringkat
- Microbial Diseases of The Cardiovascular and Lymphatic SystemsDokumen27 halamanMicrobial Diseases of The Cardiovascular and Lymphatic SystemsAbhishek Isaac MathewBelum ada peringkat
- Systematic Inflammatory Response Syndrome: Presented By: Group 1 (Acuna, Basinang, Bernardino & Lavadia)Dokumen11 halamanSystematic Inflammatory Response Syndrome: Presented By: Group 1 (Acuna, Basinang, Bernardino & Lavadia)Boch NoyBelum ada peringkat
- Severe SepsisDokumen8 halamanSevere SepsisKie SanBelum ada peringkat
- Annalsats Articles in Press. Published February 03, 2023 As 10.1513/Annalsats.202211-946OcDokumen33 halamanAnnalsats Articles in Press. Published February 03, 2023 As 10.1513/Annalsats.202211-946OcAlexandre Cavalcanti100% (1)
- Idiot NotesDokumen53 halamanIdiot NotesRay PerezBelum ada peringkat
- Antibiotic Guidelines For Adults 2018 PDFDokumen58 halamanAntibiotic Guidelines For Adults 2018 PDFAhmad RizqiBelum ada peringkat
- Screening Tool Dental Under 5 DN10060Dokumen1 halamanScreening Tool Dental Under 5 DN10060Kiranvarma KakarlapudiBelum ada peringkat
- Introduction To Critical Care NursingDokumen10 halamanIntroduction To Critical Care NursingAngielyn Ramos Oloraza100% (2)
- Management of Septic Abortion and ComplicationsDokumen19 halamanManagement of Septic Abortion and Complicationsapi-370504683% (6)
- Nursing Workload and Patient Care - 0 PDFDokumen98 halamanNursing Workload and Patient Care - 0 PDFEg RevaBelum ada peringkat
- IFHIMA Congress 2019 ProceedingsDokumen142 halamanIFHIMA Congress 2019 ProceedingsNadya AnggrainiBelum ada peringkat
- NAG Skin and Soft Tissue Infections AdultsDokumen21 halamanNAG Skin and Soft Tissue Infections AdultsJun JimenezBelum ada peringkat
- Intraoperative Vasoplegia: Methylene Blue To The Rescue!: ReviewDokumen7 halamanIntraoperative Vasoplegia: Methylene Blue To The Rescue!: ReviewSandra GarGarBelum ada peringkat
- C304 Task 1 Word A PDFDokumen33 halamanC304 Task 1 Word A PDFCamille Joy BaliliBelum ada peringkat