Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Weight-For-Age GIRLS: 2 To 5 Years (Z-Scores)Dokumen1 halamanWeight-For-Age GIRLS: 2 To 5 Years (Z-Scores)Gibson HorasBelum ada peringkat
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Management of Protozoal Diarrhoea in HIV DiseaseDokumen6 halamanManagement of Protozoal Diarrhoea in HIV DiseaseSri Nowo MinartiBelum ada peringkat
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Daftar PustakaDokumen1 halamanDaftar PustakaSri Nowo MinartiBelum ada peringkat
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Association Between Smoking Behavior and LDLDokumen1 halamanAssociation Between Smoking Behavior and LDLSri Nowo MinartiBelum ada peringkat
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Abnormal Uterine Bleeding: Frequently Asked Questions FAQ095 Gynecologic ProblemsDokumen3 halamanAbnormal Uterine Bleeding: Frequently Asked Questions FAQ095 Gynecologic ProblemsErwinBelum ada peringkat
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Nephrotic Syndrome in Adults 2009Dokumen6 halamanNephrotic Syndrome in Adults 2009Mutiara RizkyBelum ada peringkat
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Cover Skripsi Bahasa InggrisDokumen1 halamanCover Skripsi Bahasa InggrisSri Nowo MinartiBelum ada peringkat
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
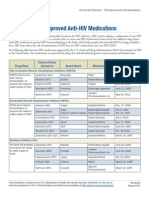
- ApprovedMedstoTreatHIV FS enDokumen2 halamanApprovedMedstoTreatHIV FS enSri Nowo MinartiBelum ada peringkat
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Eur Heart J 2003 Fröhlich 1365 72Dokumen8 halamanEur Heart J 2003 Fröhlich 1365 72Sri Nowo MinartiBelum ada peringkat
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
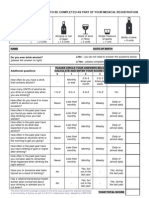
- Alcohol 10 QuestionnaireDokumen1 halamanAlcohol 10 Questionnaireyash_magooBelum ada peringkat
- Management of Protozoal Diarrhoea in HIV DiseaseDokumen6 halamanManagement of Protozoal Diarrhoea in HIV DiseaseSri Nowo MinartiBelum ada peringkat
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Nkcells Further ReadDokumen1 halamanNkcells Further ReadSri Nowo MinartiBelum ada peringkat
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- 55 259Dokumen6 halaman55 259Sri Nowo MinartiBelum ada peringkat
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Afroz - Lipid ProfileDokumen6 halamanAfroz - Lipid ProfileSri Nowo MinartiBelum ada peringkat
- Uroanalisis AnormalDokumen13 halamanUroanalisis AnormalMyke EstradaBelum ada peringkat
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Dysuria in AdultsDokumen8 halamanDysuria in AdultsSi vis pacem...Belum ada peringkat
- Frequency of Renal Stone Disease in Patients With Urinary Tract InfectionDokumen3 halamanFrequency of Renal Stone Disease in Patients With Urinary Tract InfectionSri Nowo MinartiBelum ada peringkat
- Uroanalisis AnormalDokumen13 halamanUroanalisis AnormalMyke EstradaBelum ada peringkat
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- VancouverDokumen11 halamanVancouverAndi Firman MubarakBelum ada peringkat
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Frequency of Renal Stone Disease in Patients With Urinary Tract InfectionDokumen3 halamanFrequency of Renal Stone Disease in Patients With Urinary Tract InfectionSri Nowo MinartiBelum ada peringkat
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- ResourceDokumen5 halamanResourceSri Nowo MinartiBelum ada peringkat
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- The Effect of Human Recombinant Erythropoietin On Prevention of Anemia of PrematurityDokumen6 halamanThe Effect of Human Recombinant Erythropoietin On Prevention of Anemia of PrematuritySri Nowo MinartiBelum ada peringkat
- Difco BBL Mueller Hinton Agar BrothDokumen5 halamanDifco BBL Mueller Hinton Agar BrothSri Nowo MinartiBelum ada peringkat
- Corrections: Theodore J. Cicero, Ph.D. Matthew S. Ellis, M.P.EDokumen1 halamanCorrections: Theodore J. Cicero, Ph.D. Matthew S. Ellis, M.P.ESri Nowo MinartiBelum ada peringkat
- EpoDokumen15 halamanEpoSri Nowo MinartiBelum ada peringkat
- Corrections: Theodore J. Cicero, Ph.D. Matthew S. Ellis, M.P.EDokumen1 halamanCorrections: Theodore J. Cicero, Ph.D. Matthew S. Ellis, M.P.ESri Nowo MinartiBelum ada peringkat
- Niacin MOADokumen3 halamanNiacin MOASri Nowo Minarti100% (1)
- Am J Clin Nutr 2008 Kupka 1802 8Dokumen7 halamanAm J Clin Nutr 2008 Kupka 1802 8Sri Nowo MinartiBelum ada peringkat
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Etiology and Evaluation of Diarrhea in AIDS: A Global Perspective at The MillenniumDokumen10 halamanEtiology and Evaluation of Diarrhea in AIDS: A Global Perspective at The MillenniumSri Nowo MinartiBelum ada peringkat
- Computerized Flat Knitting Machine Computerized Flat Knitting Machine Computerized Flat Knitting Machine Computerized Flat Knitting MachineDokumen61 halamanComputerized Flat Knitting Machine Computerized Flat Knitting Machine Computerized Flat Knitting Machine Computerized Flat Knitting MachineAmira's ClothesBelum ada peringkat
- 762id - Development of Cluster-7 Marginal Field Paper To PetrotechDokumen2 halaman762id - Development of Cluster-7 Marginal Field Paper To PetrotechSATRIOBelum ada peringkat
- Korea Times - Korean-EnglishDokumen313 halamanKorea Times - Korean-EnglishgyeryongBelum ada peringkat
- New - BMP3005 - ABF - Assessment Brief - FDokumen5 halamanNew - BMP3005 - ABF - Assessment Brief - Fmilka traykovBelum ada peringkat
- DU Series MCCB CatalogueDokumen8 halamanDU Series MCCB Cataloguerobinknit2009Belum ada peringkat
- 3 A Sanitary Standards Quick Reference GuideDokumen98 halaman3 A Sanitary Standards Quick Reference GuideLorettaMayBelum ada peringkat
- ФО Англ.яз 3клDokumen135 halamanФО Англ.яз 3клБакытгуль МендалиеваBelum ada peringkat
- Ultrasonic Based Distance Measurement SystemDokumen18 halamanUltrasonic Based Distance Measurement SystemAman100% (2)
- Online Shopping MallDokumen17 halamanOnline Shopping MallMerin LawranceBelum ada peringkat
- Lit 30Dokumen2 halamanLit 30ReemAlashhab81Belum ada peringkat
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Basler Electric TCCDokumen7 halamanBasler Electric TCCGalih Trisna NugrahaBelum ada peringkat
- Retail Visibility Project of AircelDokumen89 halamanRetail Visibility Project of Aircelabhishekkraj100% (1)
- Comparison of Sic Mosfet and Si IgbtDokumen10 halamanComparison of Sic Mosfet and Si IgbtYassir ButtBelum ada peringkat
- Silapathikaram 3Dokumen37 halamanSilapathikaram 3gavinilaaBelum ada peringkat
- Islcollective Present SimpleDokumen2 halamanIslcollective Present Simplecrisan mirunaBelum ada peringkat
- Model Contract FreelanceDokumen3 halamanModel Contract FreelancemarcosfreyervinnorskBelum ada peringkat
- PrimerCube Manufacturing GuideDokumen57 halamanPrimerCube Manufacturing GuideTinaMaleenaBelum ada peringkat
- Cad32gd - Contactor ManualDokumen28 halamanCad32gd - Contactor Manualhassan karimiBelum ada peringkat
- Written Report in Instructional PlanningDokumen6 halamanWritten Report in Instructional PlanningRose Aura HerialesBelum ada peringkat
- Geography NotesDokumen2 halamanGeography NotesMinethegroundBelum ada peringkat
- Hydropneumatic Booster Set MFDokumen5 halamanHydropneumatic Booster Set MFdonchakdeBelum ada peringkat
- DS SX1280-1-2 V3.0Dokumen143 halamanDS SX1280-1-2 V3.0bkzzBelum ada peringkat
- Catalogue Laboratory Products - Heraeus KulzerDokumen288 halamanCatalogue Laboratory Products - Heraeus KulzerDentaDentBelum ada peringkat
- Bakteri Anaerob: Morfologi, Fisiologi, Epidemiologi, Diagnosis, Pemeriksaan Sy. Miftahul El J.TDokumen46 halamanBakteri Anaerob: Morfologi, Fisiologi, Epidemiologi, Diagnosis, Pemeriksaan Sy. Miftahul El J.TAlif NakyukoBelum ada peringkat
- Cs Fujitsu SAP Reference Book IPDFDokumen63 halamanCs Fujitsu SAP Reference Book IPDFVijay MindfireBelum ada peringkat
- S O S Services Alert Level Help Sheet - REFERENCIALESDokumen20 halamanS O S Services Alert Level Help Sheet - REFERENCIALESDavid Poma100% (1)
- Caldon Lefm 240ci Ultrasonic Flow Meters: Integral Manifold DesignDokumen6 halamanCaldon Lefm 240ci Ultrasonic Flow Meters: Integral Manifold DesignJim LimBelum ada peringkat
- Crown BeverageDokumen13 halamanCrown BeverageMoniruzzaman JurorBelum ada peringkat
- 3.2.1 The Role of Market Research and Methods UsedDokumen42 halaman3.2.1 The Role of Market Research and Methods Usedsana jaleelBelum ada peringkat
- Journal Articles: Types of JournalsDokumen4 halamanJournal Articles: Types of JournalsOtieno SteveBelum ada peringkat
- The Obesity Code: Unlocking the Secrets of Weight LossDari EverandThe Obesity Code: Unlocking the Secrets of Weight LossPenilaian: 4 dari 5 bintang4/5 (6)
- The Age of Magical Overthinking: Notes on Modern IrrationalityDari EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityPenilaian: 4 dari 5 bintang4/5 (28)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsDari EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsBelum ada peringkat
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeDari EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BePenilaian: 2 dari 5 bintang2/5 (1)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDDari EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDPenilaian: 5 dari 5 bintang5/5 (1)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionDari EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionPenilaian: 4 dari 5 bintang4/5 (404)